Review of Normal Histology
Pathology Cases for Week 1
Normal Histology Slide Descriptions
Norm No. 1 Prostate
[ImageScope] [WebScope]
The prostate gland is composed of multiple glandular spaces lines by a basal layer of cuboidal epithelium covered by columnar secretory cells with frequent papillary projections into the gland lumen. The cells are uniform in size and shape. The nuclei are not crowded. They do not have nucleoli that are visible. Glands are separated by fibrovascular stroma.
Norm No. 2 Kidney
[ImageScope] [WebScope]
The kidney excretes soluble waste from the body and controls electrolyte balance. It consists of the cortex and the medulla. Within the outer cortex, glomeruli with delicate capillary loops are seen. The basement membrane is thin and without inflammation or thickening. Bowman’s capsule that surrounds the glomerulus is thin. The interstitium demonstrates no evidence of inflammation or fibrosis. In the areas between the glomeruli, tubules and arterioles are seen. The tubules are intact. The vessels exhibit no narrowing or wall thickening. The inner medulla of the kidney contains only tubules and blood vessels. Larger arteries and veins are located at the interface between cortex and medulla.
Norm No. 3 Liver
[ImageScope] [WebScope]
The liver is the organ that metabolizes nutrients received from the digestive tract. These nutrients and processed by tissue hepatocytes which are large polygonal cells. The hepatocyes are separated by portal triads. The triads consist of an artery, a vein and a bile duct. The bile duct is lined by cuboidal epithelium. The artery has a muscular wall and a flat endothelial lining. The sinuses are well defined and contain a small amount of blood.
Norm No. 4 Ovary
[ImageScope] [WebScope]
Ovary tissue consists of stoma which is composed of elongated stromal cells. Within the stoma are oocytes in various stages of development. Most of the oocytes have not been stimulated to mature. These resting oocytes have very large nuclei with prominent nucleoli. There are corpora albicantia in a bland stroma. The Corpus Luteum of Pregnancy is composed of granulosa cells with abundant foamy cytoplasm. The granulosa cells are arranged in complex folds.
Norm No. 5 Thyroid
[ImageScope] [WebScope]
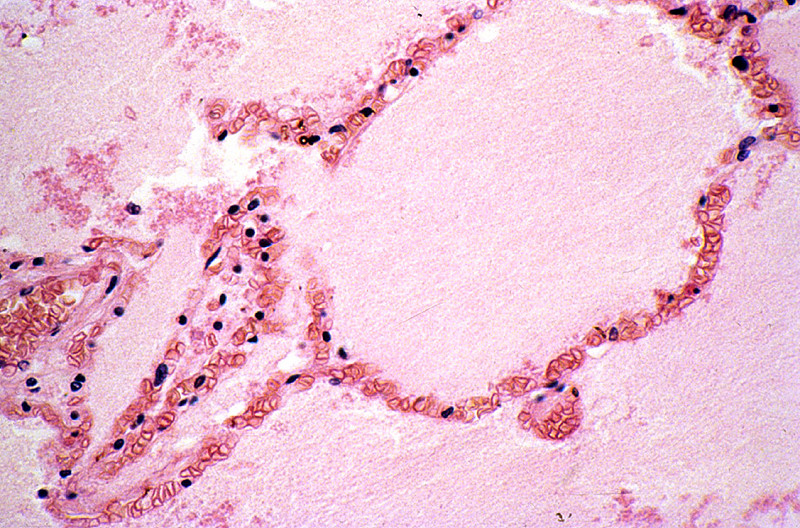
Thyroid tissue consists of variably-sized, colloid-filled follicles. The colloid is eosinophilic and homogeneous. The glandular thyroid cells are cuboidal. The capsule is intact.
Norm No. 6 Bone marrow (section)
[ImageScope] [WebScope]
Normal bone marrow is about 50% hematopoietic elements and the remainder is mature adipocytes. There is trilineage hematopoiesis present with complete maturation of all cell lines. The myeloid to erythroid ratio is approximately 3:1. Megakaryocytes are present. No lymphoid aggregates are present. The bony trabeculae appear form a normal meshwork.
Norm No. 7 Pancreas
[ImageScope] [WebScope]
The pancreas is comprised of glandular tissue with endocrine and exocrine function. The exocrine pancreas contains lobular arrays of acini. The acinar secretions of the exocrine pancreas are collected by the pancreatic ducts. The ducts are surrounded by a small amount of connective tissue without inflammation or fibrosis (scarring).The endocrine pancreas resides in the islets which are regularly arranged and present within the pancreatic lobules.
Norm No. 8 Appendix
[ImageScope] [WebScope]
The appendix is a tubular organ with a lumen which is lined by mucin secreting columnar epithelium. There is no evidence of acute inflammation. The submucosa and muscle layers are unremarkable. There is no inflammation of the serosa.
Norm No. 9 Aorta
[ImageScope] [WebScope]
The aorta is a large elastic artery. The luminal surface is lined by flat endothelial cells. This is called the “intima”. Adjacent to the intima is the internal elastic lamina. This is composed of elastin and has a corrugated appearance on histological section. Adjacent to the internal elastic lamina is the tunica media which is composed of smooth muscle. Finally, the outermost layer is the adventitia which is composed of connective tissue.
Norm No. 10 Pubic symphysis
[ImageScope] [WebScope]
The pubic symphysis includes cartilage, bone, dense connective tissue and bone as well as skeletal muscles inserting into the bone.
Norm No. 11 Adrenal gland
[ImageScope] [WebScope]
Adrenal tissue is composed of a central medulla and outer cortex. The medulla contains large polygonal neuroendocrine cells. The cortex contains cells with foamy cytoplasm. There is no evidence of hemorrhage or necrosis.
Norm No. 12 Cervix
[ImageScope] [WebScope]
Cervix tissue consists of exocervix which is exposed to the environment of the vagina. The exocervix is covered by non-keratinizing squamous epithelium. The exocervix is continuous with the endocervix via the “transition zone”. The endocervix is covered by glandular epithelium. The lining cells are mucous secreting cells. A few small glands may be seen in the cervix. The cervix proper is composed of smooth muscle. This merges imperceptibly with the smooth muscle of the myometrium.
Norm No. 13 Heart
[ImageScope] [WebScope]
Normal heart tissue sections demonstrate no evidence of fibrosis or hemorrhage. Cardiac myocytes have moderately sized centrally located nuclei. Normal myocytes are not brightly eosinphilic. Normally no inflammation is seen. Normal cardiac myocytes do not show hypertrophy.
Norm No. 14 Pituitary gland
[ImageScope] [WebScope]
The pituitary is an endocrine gland with neurohypophysis and adenohypophysis. The neurohypophysis is composed of spindle cells that are derived from neural crest. These are neurosecretory cells. The adenohypophysis is an endocrine gland which is composed of three histological cell types, acidophils, basophils and chromophobes. The staining properties vary with the hormonal product. For example, growth hormone secreting cells are acidophils.
Norm No. 15 Skin
[ImageScope] [WebScope]
Skin consists of keratinizing stratified squamous epithelium. The keratin layer is eosinophilic. Nuclei are not present. Beneath the keratin layer is a layer of flat epithelial cells with small pyknotic nuclei. Cells are regular and not crowded. These keratinocytes rest upon a layer of basal epithelium and a thin basement membrane. Beneath the epidermis is the dermis which consists of loose connective tissue. Within the dermis are sweat and sebaceous glands. Some slides contain hair follicles. There is no inflammation. The blood vessels are patent and do not contain thromboemboli.
Norm No. 16 Stomach, fundus
[ImageScope] [WebScope]
The normal gastric mucosa of the fundus contains superficial fovea arranged in leaf like fronds and deeper gastric glands. The foveolar cells secrete mucin. The gastric glands include mucous cells, parietal cells, chief cells and enteroendocrine cells.
Norm No. 17 Jejunum
[ImageScope] [WebScope]
This cross section of the jejunum illustrates the complex mucosal villi and crypts that greatly increase the absorptive surface area.
Norm No. 18 Skeletal muscle
[ImageScope] [WebScope]
Skeletal muscle fibers have striations which are easily seen on the longitudinal section. Nuclei are located at the periphery of normal striated muscle fibers.
Norm No. 19 Female breast
[ImageScope] [WebScope]
The female breast is a secretory organ that produces milk during lactation. Breast tissue that is not stimulated to lactate consists of resting apocrine cells arranged in nests and small ductules which are lined by cuboidal epithelium. The secretory units are separated from one another by loose connective tissue.
Norm No. 20 Uterine (fallopian) tube (aka oviduct)
[ImageScope] [WebScope]
The fallopian tube is lined by ciliated columnar epithelium that aid in transport of the ovum to the uterus. The epithelium is arranged in fronds that project into the lumen. The wall consists of smooth muscle and connective tissue.
Norm No. 21 Uterus
[ImageScope] [WebScope]
The uterus is a reproductive organ, capable of enormous growth during pregnancy. It is composed of an inner endometrium which supports the placenta during pregnancy. The glandular endometrium undergoes monthly cycles in response to endocrine influence. It undergoes proliferation and then a secretory phase when it is capable of supporting a fertilized ovum. It is subsequently shed during menstruation. The endometrial here is proliferative. If you look carefully you can see mitotic figures in the endometrial glands. Note the regular spacing and orderly array of the endometrial glands. Beneath the endometrium is the myometrium which is composed of smooth muscle cells.
Norm No. 22 Testis
[ImageScope] [WebScope]
The testis is the male gland responsible for sperm production. There is a fibrous capsule and multiple glands separated by a loose stoma. Within the glands there are mature and immature sperm. Within the stroma there are a few large Leydig cells which are responsible for testosterone production.
Norm No. 23 Epididymis
[ImageScope] [WebScope]
The epididymis is a narrow, tightly-coiled tube connecting the efferent ducts from the rear of each testicle to its vas deferens. Each of the ducts is lined by ciliated columnar epithelium that aid in transport of the sperm for ejaculation. Some of the larger ducts are filled with sperm.
Norm No. 24 Lung
[ImageScope] [WebScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
Norm No. 25 Spleen
[ImageScope] [WebScope]
The spleen is a composed mostly of lymphocytes in a loose blood filled stroma with islands of fibrous tissue. Surrounding the spleen is a dense connective tissue capsule.
Norm No. 26 Trachea
[ImageScope] [WebScope]
The trachea is lined by ciliated columnar epithelium. Within the submucosa are mucous glands. Under the glands is the cartilage that gives the trachea strength.
Norm No. 27 Colon
[ImageScope] [WebScope]
Colon is lined by glandular epithelium with numerous mucin secreting goblet cells. The epithelium is arranged in folds to increase the surface area available for absorption.
Norm No. 28 Submandibular and sublingual salivary glands
[ImageScope] [WebScope]
The submandibular and sublingual salivary glands are sero-mucous exocrine glands, meaning they produce a mixture of serous (watery and proteinaceous) and mucous (viscous and carbohydrate rich) secretions. The submandibular gland is mostly serous whereas the sublingual gland is mostly mucous. There are nests of cells which produce saliva as well as ducts which transport the saliva to the oral cavity. Note the regular orderly array of cells and stroma.
Norm No. 29 Lymph node
[ImageScope] [WebScope]
The lymph node contains a cortex which includes the lymphoid follicles and a medulla which is looser tissue containing the lymphatic channels and blood vessels.
Norm No. 30 Cerebellum
[ImageScope] [WebScope]
This section of cerebellum is from the vermis. The cerebellum is arranged in complex folds called folia. Each folium has a relatively acellular molecular layer, a Purkinje cell layer which contains large Prukinje neurons, a molecular layer which contains small neurons and glia and white matter, which is stained blue in this hematoxylin and eosin/luxol fast blue stained preparation.
Norm No. 31 Urinary bladder
[ImageScope] [WebScope]
The urinary bladder is composed of thick smooth muscle and lined by transitional epithelium.
Pathology Case Descriptions
CASE NUMBER 31
[ImageScope] [WebScope]
Clinical History: This 45-year-old man had been well until he was awakened by chest pain that radiated to both arms and neck and was associated with diaphoresis. His blood pressure was 160/110. He was treated with diuretics (Lasix), but he continued to gain weight. Two days after the onset of the chest pain he had a cardiac arrest and died.
Image Gallery:
(Summary of Gross Findings - click here)
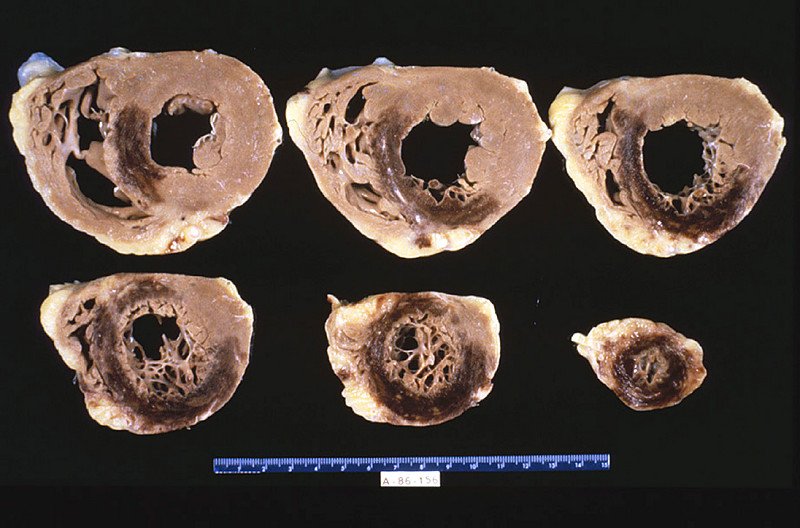
The heart was slightly enlarged weighing 460gms. There was severe atherosclerosis of all the major coronary arteries with a recent thrombotic occlusion of the proximal left anterior descending coronary artery. A recent transmural infarct was present in the left ventricle that involved the interventricular septum and the papillary muscle.
|
(Summary of Microscopic Findings - click here)
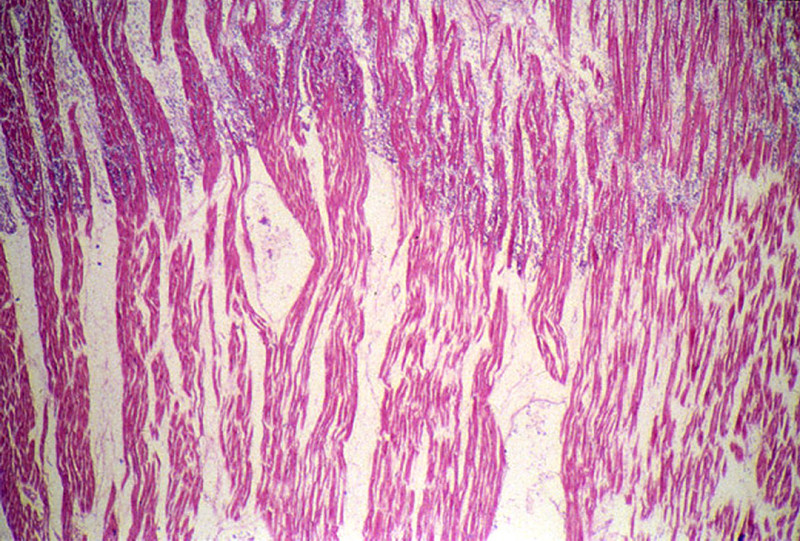
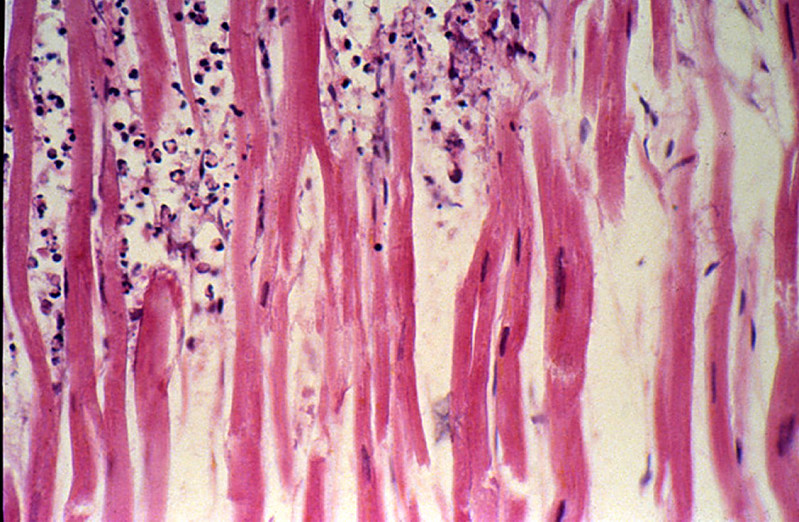
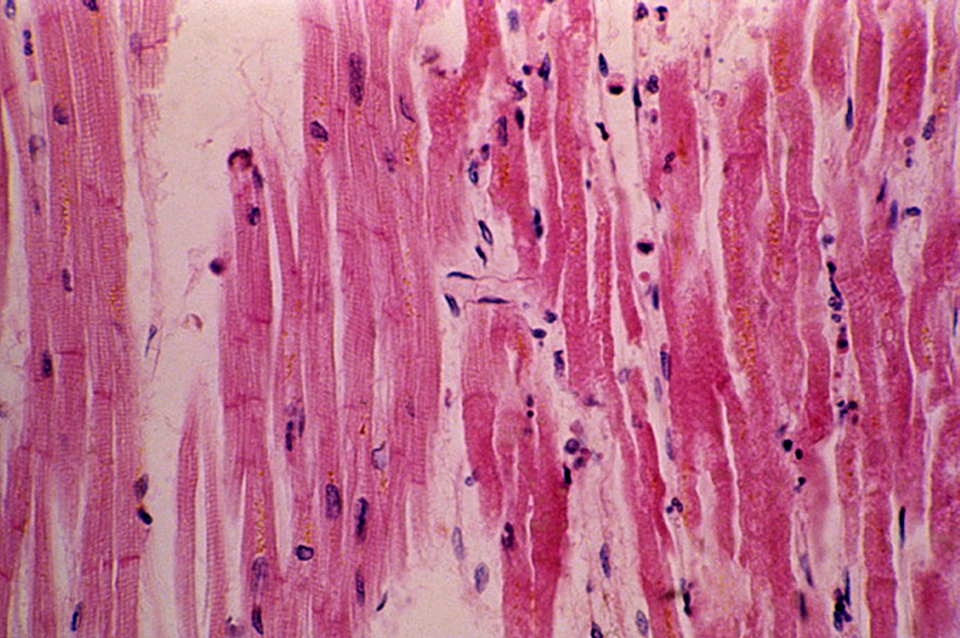
The slide includes a transmural section of the left ventricle. Nearly the entire section is involved by infarct. However, there is a thin rim (5 to 10 cell layers) of endocardial myocytes which have survived because of diffusion of oxygen and nutrients from the ventricular cavity. Other viable myocytes can be found around larger blood vessels within the section. The intense hypereosinophilia of the necrotic myocytes can best be appreciated by comparing the thin rim of lighter staining subendocardial myocytes with the deeper cells. Note also the karyolysis that is characteristic of coagulation necrosis. In some areas there is little inflammatory response. This observation is explained by microvascular necrosis which does not allow access of circulating leukocytes to these areas. In other areas, especially in the epicardial half of the infarct, there is an intense acute inflammatory response. Many intact neutrophils can be seen. In addition, there are many nuclear fragments from lysed neutrophils. Macrophage activity is not evident. These features of the inflammatory response indicate that the infarct was approximately three to four days old. Note also that the inflammation extends to the epicardial surface and that there are deposits of fibrin on the epicardium. This is called fibrinous pericarditis. The granular grey material seen within some blood vessels is barium sulfate, which was injected to permit post-mortem study of the coronaries by radiography.
|
(Review Normal Histology - click here)
Norm No. 13 Heart
[ImageScope] [WebScope]
Normal heart tissue sections demonstrate no evidence of fibrosis or hemorrhage. Cardiac myocytes have moderately sized centrally located nuclei. Normal myocytes are not brightly eosinphilic. Normally no inflammation is seen. Normal cardiac myocytes do not show hypertrophy.
|
What is BEST describes the pathology observed?
ANSWER
31-1. What microscopic feature BEST describes what happened to the nuclei?
- Pyknosis
- Karyorrhexis
- Karyolysis
- Apoptosis
ANSWER
31-2. What molecular events MOST LIKELY led to the increase eosin staining of the dead myocytes?
- Loss of ribosomes
- Protein denaturation
- Protein synthesis
- A & B
ANSWER
31-3. What microscopic feature in this patient indicates that this infarct is at least 24 hours old?
- Coagulation necrosis & loss of nuclei
- Wavy fibers
- Macrophage infiltrate
- Granulation tissue
ANSWER
CASE NUMBER 14
[ImageScope] [WebScope]
Clinical History: This 37-year-old female attempted suicide by ingesting about a dozen tablets of mercury bichloride (HgCl2). A small amount of urine obtained on the first day after taking the pills was positive for occult blood. Despite vomiting, treatment with chelating agents, fluids, and colonic irrigations she became anuric and died 10 days later.
Image Gallery:
(Summary of Gross Findings - click here)
The kidneys were both slightly enlarged but grossly normal.
|
(Summary of Microscopic Findings - click here)
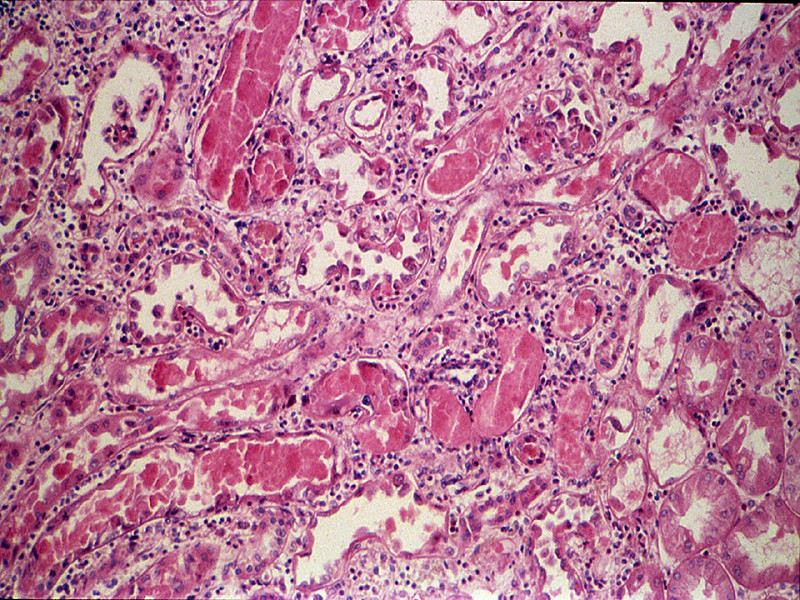
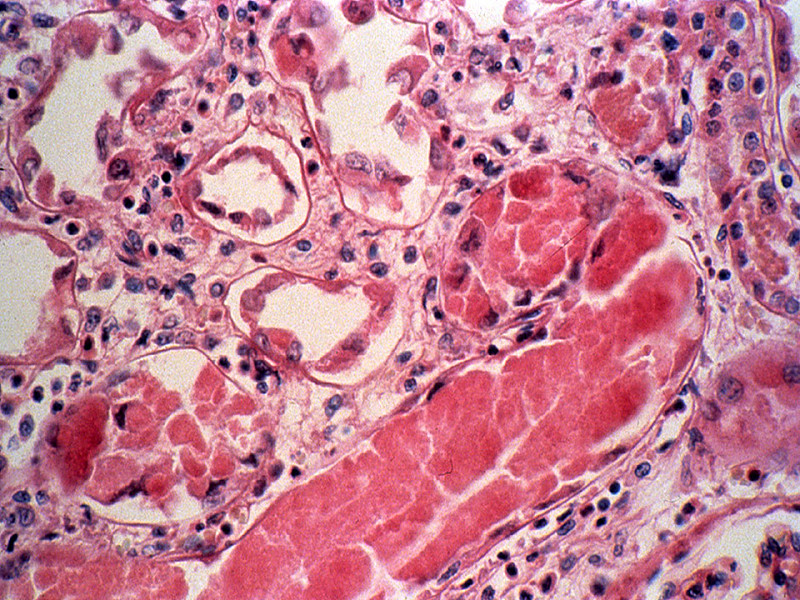
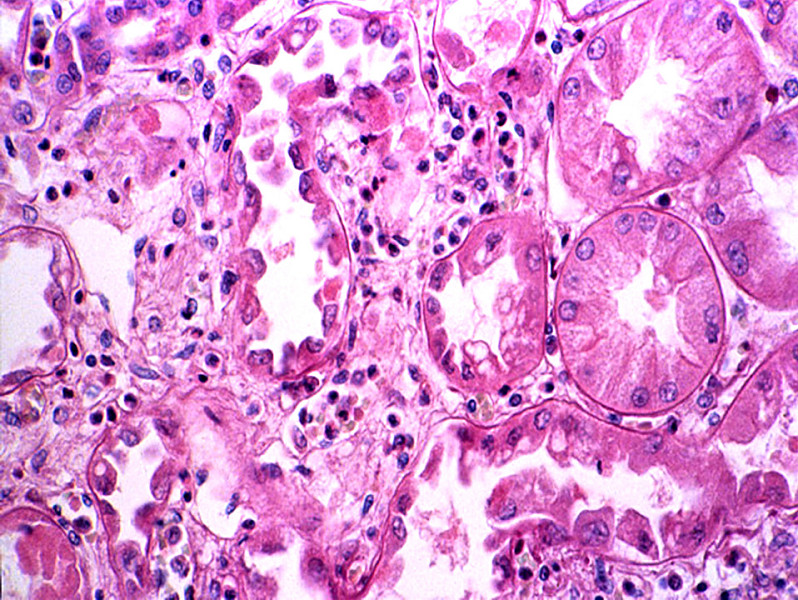
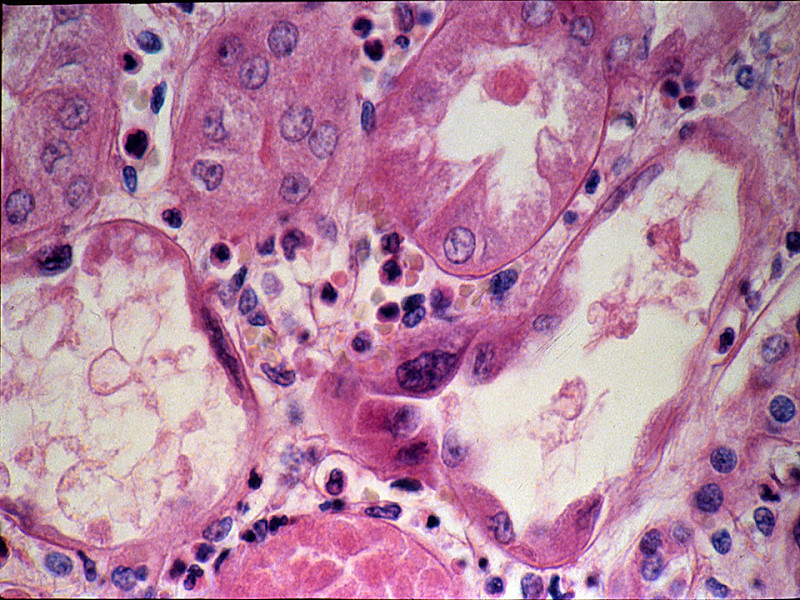
The tubular damage here is so severe that it is hard to identify the segment involved. However, it may be noted that most of the necrosis is in the cortex, whereas the collecting tubules in the medulla, although their lumina contain many casts, are lined by relatively intact cells. HgCl2 presumably damages mainly proximal convoluted tubules because it is concentrated in this segment. Many involved tubules show marked coagulative necrosis, with sloughing of cells into the lumen. Some tubules that look more nearly normal actually have already have undergone marked necrosis and all that is left is a layer of flattened basilar cells which serve to regenerate the tubule. Regenerative changes can be recognized, including occasional mitoses in epithelial cells. The basement membrane around a few necrotic tubules is broken, and the interstitial tissue contains collections of inflammatory cells and edema fluid.
|
(Review Normal Histology - click here)
Norm No. 2 Kidney
[ImageScope] [WebScope]
The kidney excretes soluble waste from the body and controls electrolyte balance. It consists of the cortex and the medulla. Within the outer cortex, glomeruli with delicate capillary loops are seen. The basement membrane is thin and without inflammation or thickening. Bowman’s capsule that surrounds the glomerulus is thin. The interstitium demonstrates no evidence of inflammation or fibrosis. In the areas between the glomeruli, tubules and arterioles are seen. The tubules are intact. The vessels exhibit no narrowing or wall thickening. The inner medulla of the kidney contains only tubules and blood vessels. Larger arteries and veins are located at the interface between cortex and medulla.
|
14-1. Given that cells that concentrate toxic molecules are most vulnerable to injury, what part of the nephron is MOST LIKELY to be damaged by mercuric chloride?
- Glomerulus
- Proximal tubule
- Loop of Henle
- Distal tubule
ANSWER
CASE NUMBER 95
[ImageScope] [WebScope]
Clinical History: A 60-year-old white male had a resection of the right side of colon for
adenocarcinoma. Seven days after the operation he had continuous abdominal discomfort and went into shock. A laparotomy revealed that the entire small bowel was gangrenous.
Image Gallery:
(Summary of Gross Findings - click here)
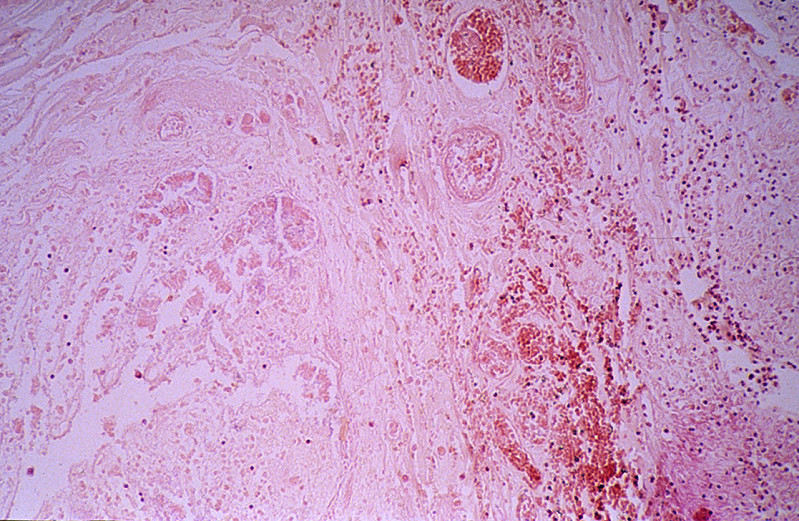
The jejunum and ileum were dark red, thickened and indurated. The mucosal surface was covered by bloody mucus. The cut surface revealed hemorrhages throughout all layers of the intestinal wall. The superior mesenteric vein and its tributaries were obstructed by dark red thrombi which were attached to the vascular wall.
|
(Summary of Microscopic Findings - click here)
The villi are swollen. The superficial layer of the mucosa is necrotic and contains clumps of bacteria. The deeper layer of the mucosa is hemorrhagic but epithelial cells are relatively well preserved. A severe degree of edema, congestion and hemorrhage is seen throughout the submucosa and muscularis layers. The muscle cells are not yet necrotic.
|
(Review Normal Histology - click here)
Norm No. 17 Jejunum
[ImageScope] [WebScope]
This cross section of the jejunum illustrates the complex mucosal villi and crypts that greatly increase the absorptive surface area.
|
What is the MOST LIKELY diagnosis?
ANSWER
95-1. The patient developed sepsis and blood culture grew a Gram negative organism. Which of the following is the most likely cause?
- The patient developed concomitant pneumonia
- There is translocation of gut bacteria
- The patient has a urinary tract infection
- The surgeon had left surgical gauze in the abdomen
ANSWER
95-2. Which of the following is the LEAST likely sequelae of venous thrombosis?
- Usually results in congestion and hemorrhage without tissue infarction
- May result in pulmonary embolism
- May propagate along the blood vessel
- May result in multiple cerebral infarcts
ANSWER
CASE NUMBER 158
[ImageScope] [WebScope]
Clinical History: A 63-year-old African American male had a five year history of progressive weakness and congestive heart failure. He complained of severe chest pain and dyspnea and died suddenly.
Image Gallery:
(Summary of Gross Findings - click here)
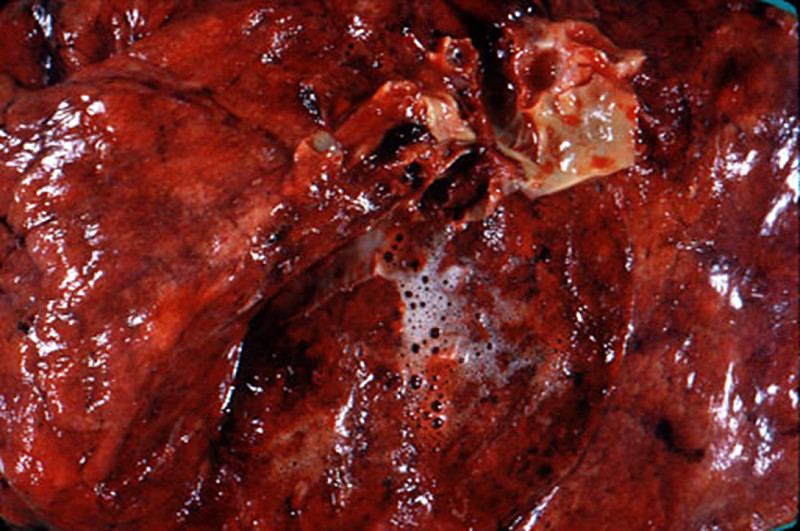
The left lung was dark red and heavy, and a large amount of hemorrhagic frothy fluid exuded freely from the cut surface. In the main pulmonary artery there was a large red firm clot adherent to the vascular wall. Many small blood clots were present in the vessels of the upper and lower lobes. Associated with these were many wedge-shaped, dark red, firmer areas in the lung parenchyma.
|
(Summary of Microscopic Findings - click here)
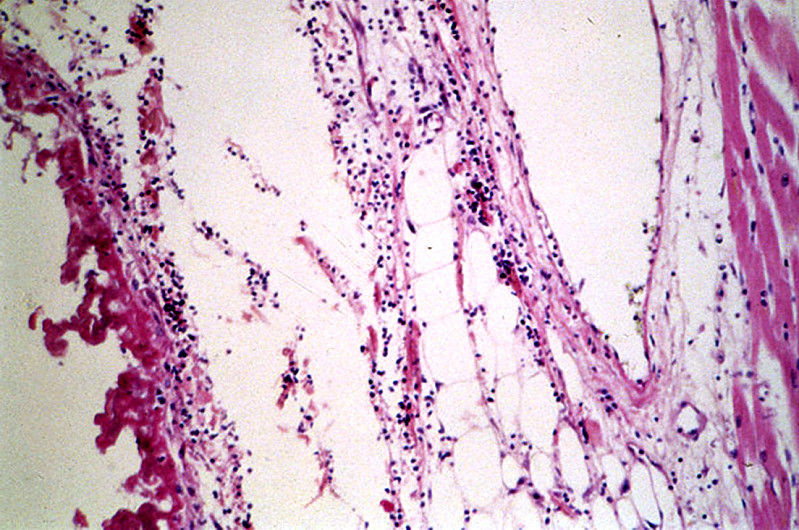
There are two sections on this slide. In the section on the right there are organizing thrombi in the pulmonary arteries. The section on the left contains a large hemorrhagic area in which some alveolar septa are pink, smudgy, and necrotic. In other portions of the sections the septa are thickened with fibrosis.
|
(Review Normal Histology - click here)
Norm No. 24 Lung
[ImageScope] [WebScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
|
What is the MOST LIKELY diagnosis?
ANSWER
158-1. In this patient, thrombi had formed in his leg veins and traveled to his lungs (pulmonary emboli). What blood vessels were occluded?
- Bronchial arteries
- Bronchial veins
- Pulmonary arteries
- Pulmonary veins
ANSWER
158-2. Why do patients have pulmonary emboli more commonly than infarcts in their lungs?
- Oxygenation from alveoli
- Dual arterial supply
- Dual venous drainage
- A & B
ANSWER
158-3. What are the firm, red wedged-shaped areas in the lung?
- Pulmonary hemorrhage
- Pulmonary infarcts
- Pulmonary metastasis
- Pulmonary angiosarcoma
ANSWER
CASE NUMBER 40
[ImageScope] [WebScope]
Clinical History: A 45-year-old male entered the hospital two days prior to death for evaluation of shortness of breath. He was found dead by the nurse.
Image Gallery:
(Summary of Gross Findings - click here)
Both lungs were heavy, wet, slightly firm, and dark-red. Frothy clear fluid may be seen on the cut surface.
|
(Summary of Microscopic Findings - click here)
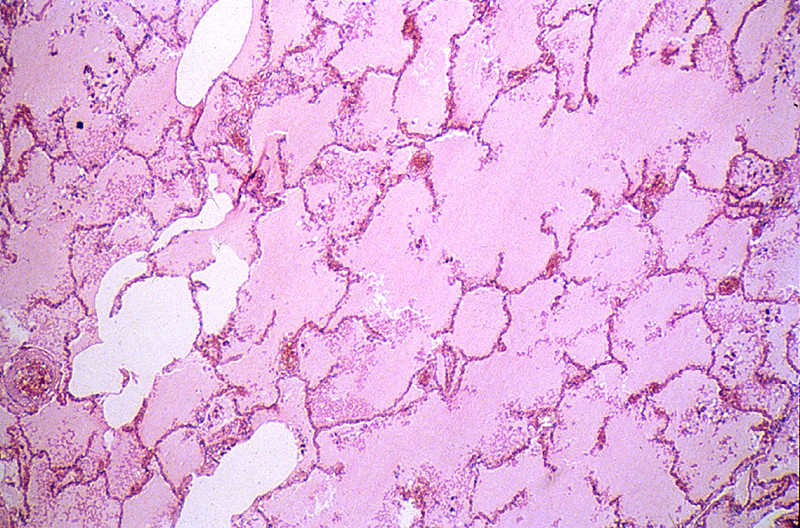
The alveoli are filled with a homogeneous pink material. The septal capillaries are engorged with blood. An incidental finding consists of anthracotic pigment near the pleural space.
|
(Review Normal Histology - click here)
Norm No. 24 Lung
[ImageScope] [WebScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
|
What is the MOST LIKELY diagnosis?
ANSWER
40-1. Causes of pulmonary edema include:
- Left heart failure
- Tricuspid stenosis
- Right heart failure
- Pulmonary thromboembolism
- NONE of the above
ANSWER
40-2. With regard to edema formation,
- ankle swelling is a sign of left heart failure
- sacral edema is a sign of right heart failure
- pulmonary edema is a sign of right heart failure
- periorbital edema is a sign of left heart failure
ANSWER
CASE NUMBER 85
[ImageScope] [WebScope]
Clinical History: This 64-year-old white female was morbidly obese.
Image Gallery:
(Summary of Gross Findings - click here)
The liver weighed 1980 grams. It had a pale, greasy appearance.
|
(Summary of Microscopic Findings - click here)
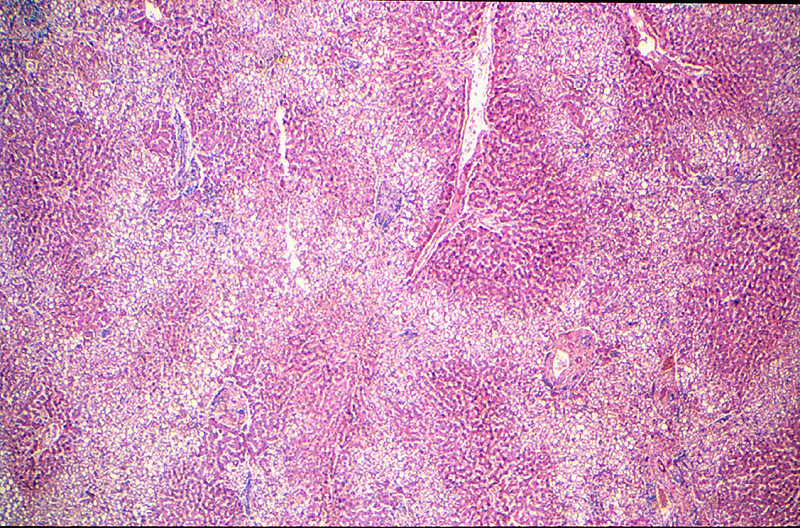
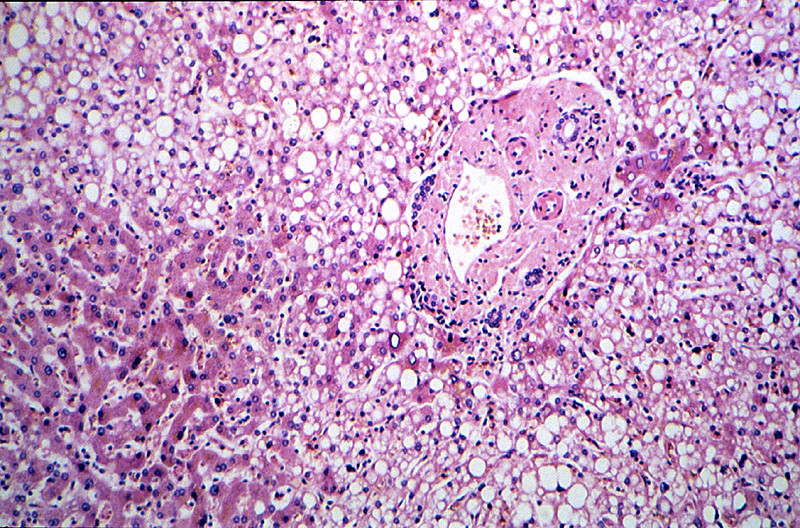
The areas of fatty change are readily visible with use of scanning power. They are zonal. Note the peri-portal areas are severely involved and the areas of fatty change extend from one portal area to another. The more severely involved cells have eccentric nuclei and the entire cytoplasm is replaced by a fat globule.
|
(Review Normal Histology - click here)
Norm No. 3 Liver
[ImageScope] [WebScope]
The liver is the organ that metabolizes nutrients received from the digestive tract. These nutrients and processed by tissue hepatocytes which are large polygonal cells. The hepatocyes are separated by portal triads. The triads consist of an artery, a vein and a bile duct. The bile duct is lined by cuboidal epithelium. The artery has a muscular wall and a flat endothelial lining. The sinuses are well defined and contain a small amount of blood.
|
85-1. What is the MOST LIKELY diagnosis?
- Metastatic carcinoma
- Cirrhosis
- Fatty liver
- Intrahepatic bile stasis
ANSWER
85-2. What of the following is the LEAST likely to cause this condition?
- Excessive alcohol consumption
- Malnutrition
- Catabolic state from cancer
- Chronic right heart failure
ANSWER
85-3. If a thin CEO were to develop this disease, you would MOST LIKELY suspect:
- Excessive alcohol consumption
- Malnutrition
- Catabolic state from cancer
- Chronic right heart failure
ANSWER
CASE NUMBER 93
[ImageScope] [WebScope]
Clinical History:A 50-year-old female had recurrent bouts of severe abdominal pain accompanied by elevated serum amylase. After one of these episodes, she developed refractory shock, peritonitis and expired.
Image Gallery:
(Summary of Gross Findings - click here)
Fibrosis obscured some areas of pancreas architecture. Saponification of peripancreatic fat was seen in small foci.
|
(Summary of Microscopic Findings - click here)
Several areas of fat necrosis with adjacent neutrophil infiltrate are seen, evidence of acute pancreatitis. In addition, some lobules of the pancreas show fibrosis and loss acini, evidence of chronic pancreatitis. In these areas, islets of Langerhans appear larger and more abundant. This is partly because they are resistant to injury and persist when acini are destroyed and partly because they undergo reactive hyperplasia.
|
(Review Normal Histology - click here)
Norm No. 7 Pancreas
[ImageScope] [WebScope]
The pancreas is comprised of glandular tissue with endocrine and exocrine function. The exocrine pancreas contains lobular arrays of acini. The acinar secretions of the exocrine pancreas are collected by the pancreatic ducts. The ducts are surrounded by a small amount of connective tissue without inflammation or fibrosis (scarring).The endocrine pancreas resides in the islets which are regularly arranged and present within the pancreatic lobules.
|
What is the MOST LIKELY diagnosis?
ANSWER
CASE NUMBER 143
[ImageScope] [WebScope]
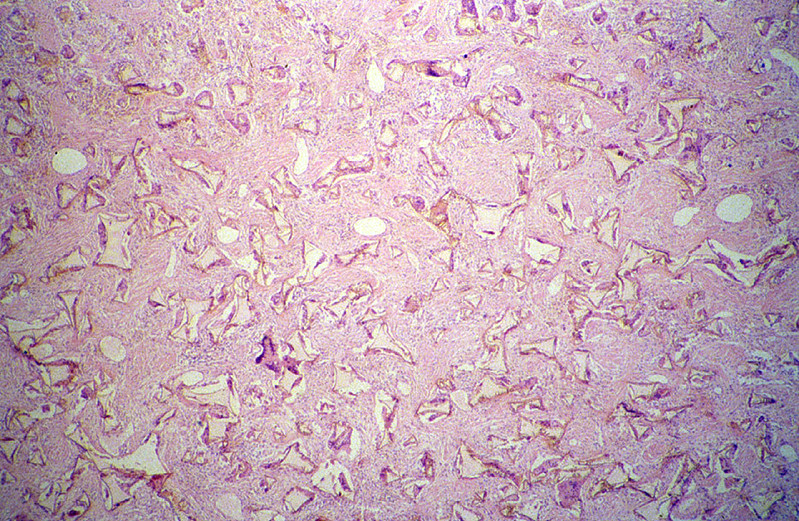
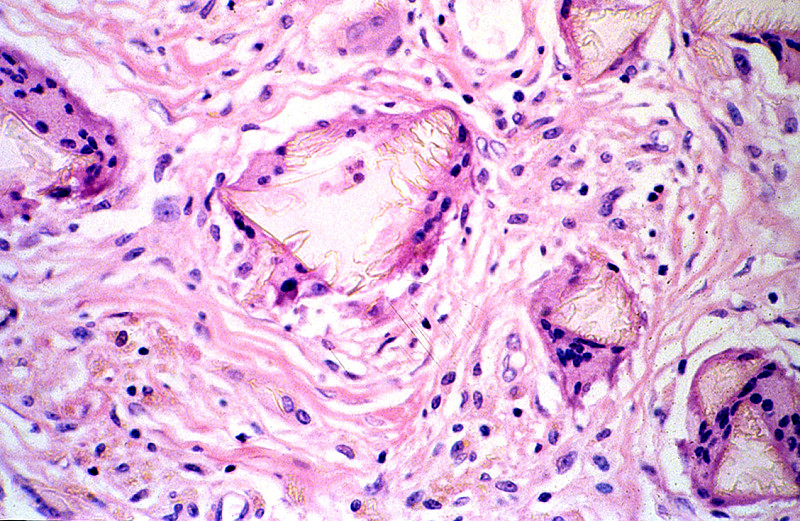
Clinical History: This 21-year-old woman desired breast enhancement. Silicone implants were placed. One of the implants ruptured causing severe inflammation and had to be removed.
Image Gallery
(Summary of Gross Findings - click here)
The cyst cavity that that surrounded the implant in the body and an example of a commonly used silicone breast implant is shown. The intact implant causes a proliferation of connective tissue that surrounds it. If the implant ruptures or leaks, the silicone causes a foreign body reaction.
|
(Summary of Microscopic Findings - click here)
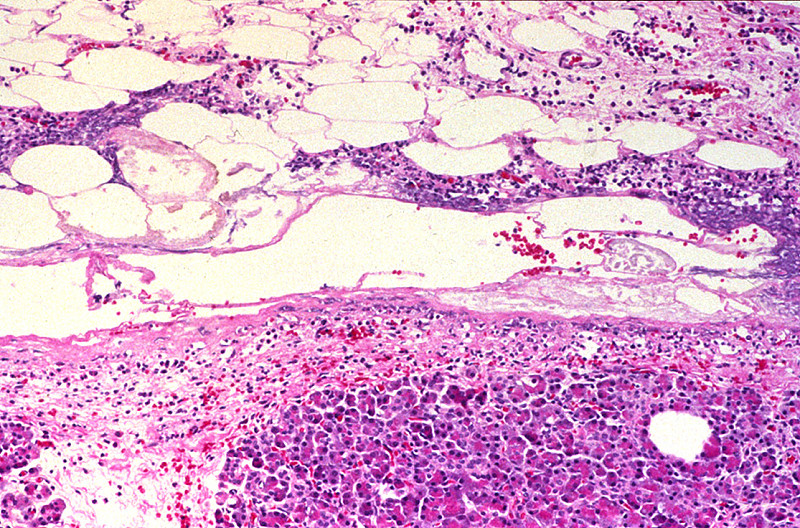
The irregular fragments of foreign material are surrounded or engulfed by multinucleated foreign body giant cells. The rest of the section is made up of fibrous connective tissue and collections of lymphocytes and histiocytes (macrophages).
|
(Review Normal Histology - click here)
Norm No. 19 Female breast
[ImageScope] [WebScope]
The female breast is a secretory organ that produces milk during lactation. Breast tissue that is not stimulated to lactate consists of resting apocrine cells arranged in nests and small ductules which are lined by cuboidal epithelium. The secretory units are separated from one another by loose connective tissue.
|
What is the MOST LIKELY diagnosis?
ANSWER
143-1. What type of inflammation is this?
- Acute inflammation
- Chronic inflammation
- Granulomatous inflammation
- Allergic inflammation
- This not an infection, therefore this is not inflammation
ANSWER
Review Items
CELL INJURY
Key Vocabulary Terms
| anthracosis |
hemosiderosis |
ischemia |
| aplasia |
heterophagy |
karyolysis |
| apoptosis |
homeostasis |
karyorrhexis |
| atrophy |
hyaline |
lipofuscin |
| autolysis |
hydropic change |
melanin |
| autophagy |
hyperplasia |
metaplasia |
| bilirubin |
hypertrophy |
necrosis |
| dysplasia |
hypoplasia |
neoplasia |
| gangrene |
hypoxia |
pyknosis |
| heat-shock protein |
infarct |
steatosis |
| hemosiderin |
|
|
CELL INJURY LEARNING OBJECTIVES
Absolutely critical information you must know to practice medicine is in bold font.
Important information that will be needed for routine patient care is in regular font.
Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics.
- Compare cell and tissue adaptation, reversible cell injury, and irreversible cell injury (cell death) on the basis of:
- etiology
- pathogenesis
- ultrastructural and histologic appearance
- Compare and contrast cell death and somatic death, on the basis of:
- causes
- pathogenesis
- histologic appearance
- Outline the relationships between the following features in terms of changes in the processes of cell injury and death:
- biochemical
- light microscopic
- ultrastructural
- Contrast and compare the clinical and pathologic features of:
- Coagulative necrosis
- liquefactive necrosis
- gangrenous necrosis
- caseous necrosis
- fat necrosis
- fibrinoid necrosis
- apoptosis
- Compare and contrast the following types of cell injury:
- reperfusion
- free radical-induced
- chemical
- understand biochemical and molecular mechanisms
- List the alterations that occur in these subcellular organelles as a consequence of cell injury:
- lysosomes
- endoplasmic reticulum
- mitochondria
- cytoskeleton
- Discuss the significance of intracellular accumulations of:
- lipids
- proteins
- glycogen
- exogenous and endogenous pigments
- Compare fatty change (steatosis) and fatty infiltration on the basis of:
- causes
- pathogenesis
- organs commonly involved
- histologic appearances
- Compare dystrophic and metastatic calcification in terms of:
- definition
- etiology and pathogenesis
- morphologic appearance
- sites and associated diseases
- clinical significance
|