Pathology Cases for Week 3
Microbiology Cases for Week 3
Pathology Case Descriptions
CASE NUMBER 35
[ImageScope] [WebScope]
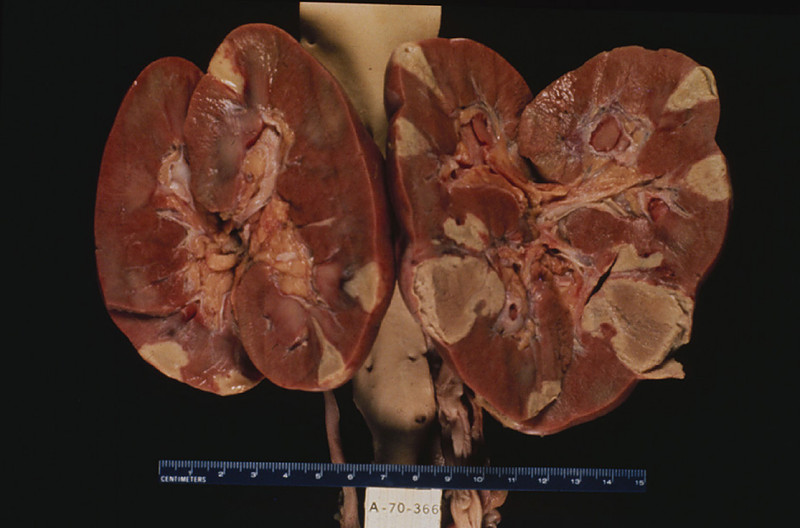
Clinical History: This was a 26-year-old female with congenital heart disease. She presented to the emergency room complaining of chest and flank pain. She developed ventricular tachycardia soon after admission and expired.
Image Gallery:
(Summary of Gross Findings - click here)
Recent infarcts are seen in the kidneys.
|
(Summary of Microscopic Findings - click here)
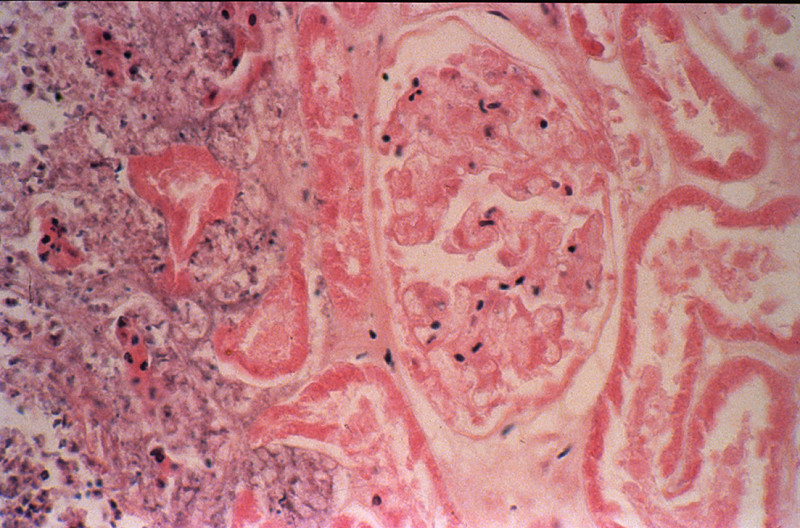
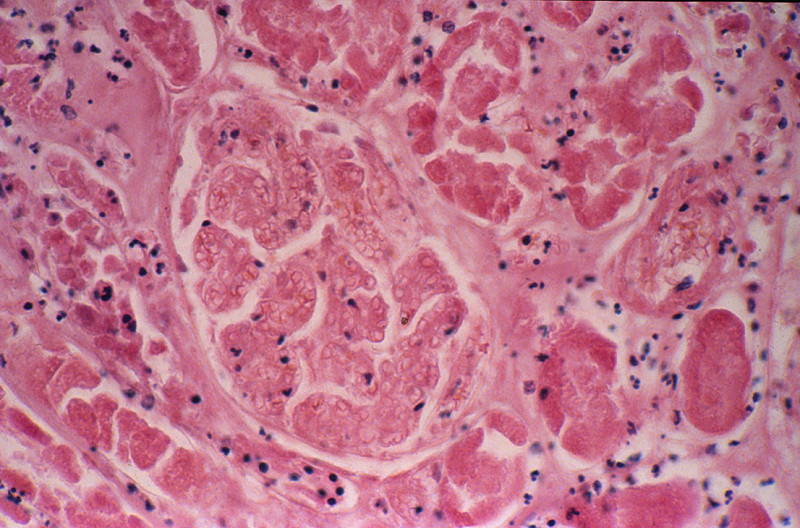
There is recent infarct in this section, with a central area containing "ghosts" of tubules outlined by a marginal zone of polymorphonuclear neutrophils, necrotic debris, and hemorrhage. Some tubules immediately beneath the renal capsule are spared. An artery in the medulla contains a thrombo-embolus that presumably originated from the thrombus on the mitral valve.
|
(Review Normal Histology - click here)
Norm No. 2 Kidney
[ImageScope] [WebScope]
The kidney excretes soluble waste from the body and controls electrolyte balance. It consists of the cortex and the medulla. Within the outer cortex, glomeruli with delicate capillary loops are seen. The basement membrane is thin and without inflammation or thickening. Bowman’s capsule that surrounds the glomerulus is thin. The interstitium demonstrates no evidence of inflammation or fibrosis. In the areas between the glomeruli, tubules and arterioles are seen. The tubules are intact. The vessels exhibit no narrowing or wall thickening. The inner medulla of the kidney contains only tubules and blood vessels. Larger arteries and veins are located at the interface between cortex and medulla.
|
|
35-1. What is the BEST explanation for the pathology demonstrated?
- Sudden drop in blood pressure
- Multiple thrombo-emboli
- Renal artery thrombosis
- Malignant hypertension
ANSWER
35-2. The appearance of the infarcts as depicted in this slide is BEST described as:
- Venous infarcts
- Arterial infarcts
- Hemorrhagic infarcts
- Lacunar infarcts
ANSWER
CASE NUMBER 370 - slide courtesy of UMich
[ImageScope] [WebScope]
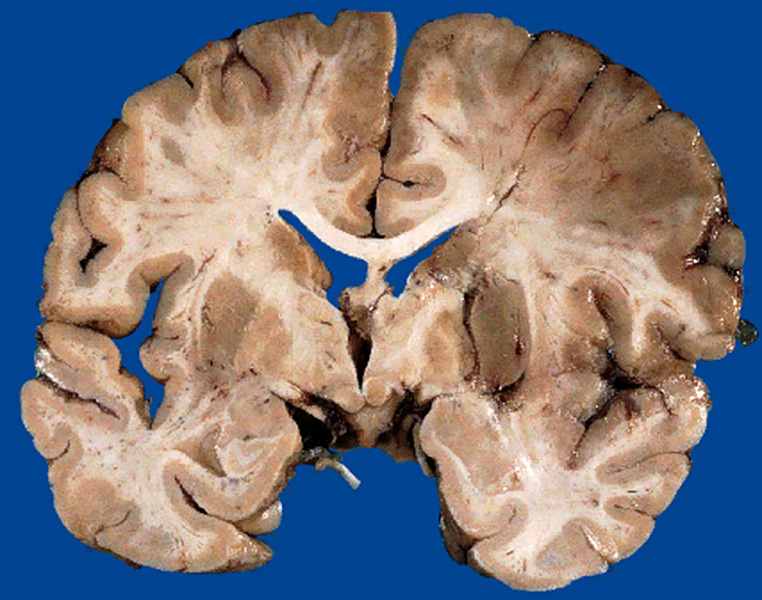
Clinical History: The patient was a 67-year-old white female who became disoriented and confused 17 days prior to death and developed paresis on the left side of the body.
Image Gallery:
(Summary of Gross Findings - click here)
There is a recent infarct in the right middle cerebral artery territory which involved the primary motor cortex as well as the lenticulostriate arteries serving the putamen, caudate, and internal capsule.
|
(Summary of Microscopic Findings - click here)
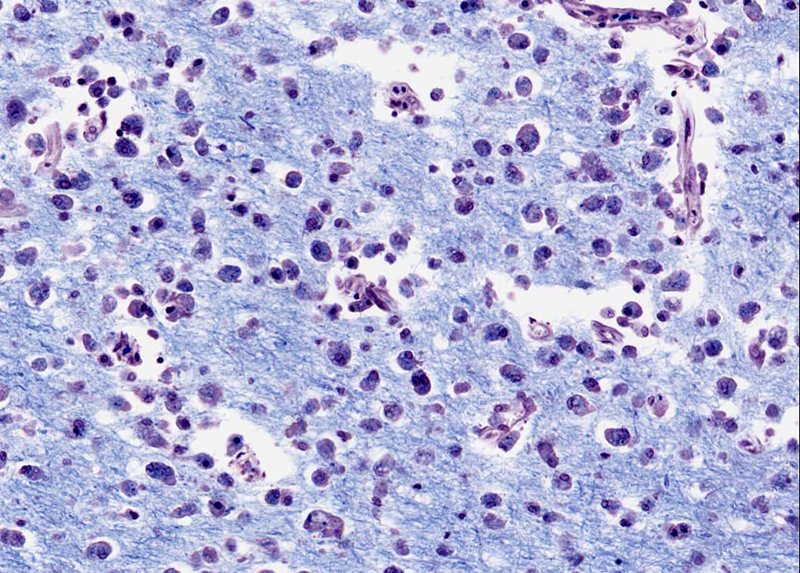
There is an area of liquefactive necrosis in the infarcted cerebral cortex. The myelin in this area stains pale due to surrounding edema fluid. The blood vessels are congested and there is some extravasated blood. (Luxol blue stain)
|
(Review Normal Histology - click here)
Cerebrum
Slide 76 (cerebrum, luxol blue/cresyl violet) [WebScope] [ImageScope]
Slide 76b (toluidine blue & eosin) [WebScope] [ImageScope]
The cerebral cortex is loosely stratified into layers containing scattered nuclei of both neurons and glial cells. Examine the layered organization of the cerebral cortex using slide 76 stained with luxol blue/cresyl violet [ORIENTATION] (which stains white matter tracts and cell bodies) or toluidine blue and eosin [ORIENTATION] (TB&E, toluidine blue stains the nuclei and RER of cells whereas eosin stains membranes and axon tracts). Typically one or more sulci (infoldings) will extend inward from one edge of the section. Examine the gray matter on each side of the sulcus using first low and then high power. Neurons of the cerebral cortex are of varying shapes and sizes, but the most obvious are pyramidal cells. As the name implies, the cell body is shaped somewhat like a pyramid, with a large, branching dendrite extending from the apex of the pyramid toward the cortical surface, and with an axon extending downward from the base of the pyramid. In addition to pyramidal cells, other nuclei seen in these sections may belong to other neurons or to glial cells also present in the cortex. You may be able to see subtle differences in the distribution of cell types in rather loosely demarcated layers. There are 6 classically recognized layers of the cortex:
- Outer plexiform (molecular) layer: sparse neurons and glia
- Outer granular layer: small pyramidal and stellate neurons
- Outer pyramidal layer: moderate sized pyramidal neurons (should be able to see these in either luxol blue [example] or TB&E-stained [example] sections)
- Inner granular layer: densely packed stellate neurons (usually the numerous processes aren’t visible, but there are lots of nuclei reflecting the cell density)
- Ganglionic or inner pyramidal layer: large pyramidal neurons (should be able to see these in either luxol blue [example] or TB&E-stained [example] sections)
- Multiform cell layer: mixture of small pyramidal and stellate neurons
Pyramidal cells in layers III and V tend to be larger because their axons contribute to efferent projections that extend to other regions of the CNS –pyramidal neurons in layer V of motor cortices send projections all the way down to motor neurons in the spinal cord!
Deep to the gray matter of the cerebral cortex is the white matter that conveys myelinated fibers between different parts of the cortex and other regions of the CNS. Be sure you identify the white matter in both luxol blue [example] and TB&E-stained [example] sections, as it will appear differently in these two stains. Review the organization of gray and white matter in cerebral cortex vs. spinal cord.
|
|
What is the MOST LIKELY diagnosis?
ANSWER
370-1. Cerebral edema may be seen in:
- A motorcyclist involved in a road traffic accident
- A 50-year old man who developed a cerebral infarct from atheromatous occlusion of the left middle cerebral artery
- A 65-year old woman with a long standing history of hypertension who developed cerebral hemorrhage
- ALL of the above
ANSWER
370-2. Which of the following may be observed in the setting of increased intracranial pressure?
- Transtentorial herniation of the cingulate gyrus
- Increased heart rate (tachycardia) and hypotension
- Unilateral dilated pupil
- Uncal herniation through the foramen magnum
- ALL of the above
ANSWER
370-3. The large, foamy cells shown in the last image in the gallery above are:
- Neurons
- Macrophages
- Neutrophils
- Lymphocytes
ANSWER
CASE NUMBER 54
[ImageScope] [WebScope]
Clinical History: An 18-year-old female had nausea, vomiting, periumbilical and lower abdominal pain, shaking chills and fever beginning two days ago. The WBC count was 21,900. Physical examination revealed local tenderness and rigidity with rebound pain in the lower abdomen. A surgical procedure was performed.
Image Gallery:
(Summary of Gross Findings - click here)
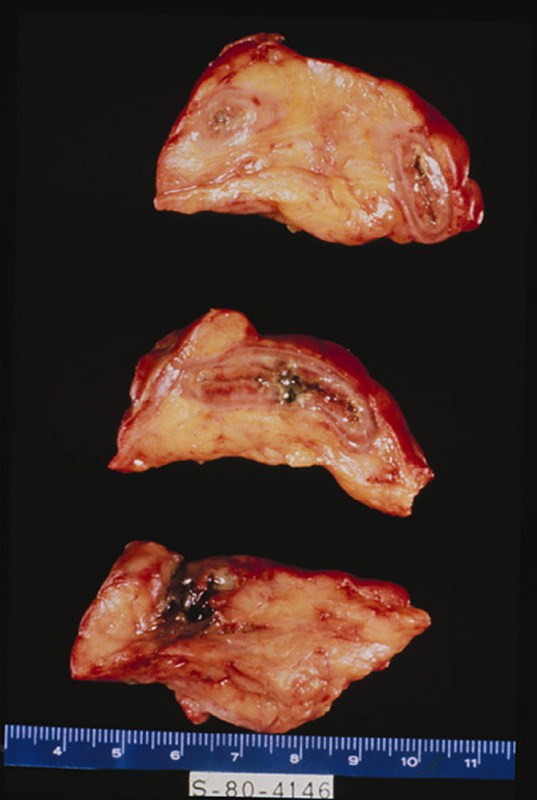
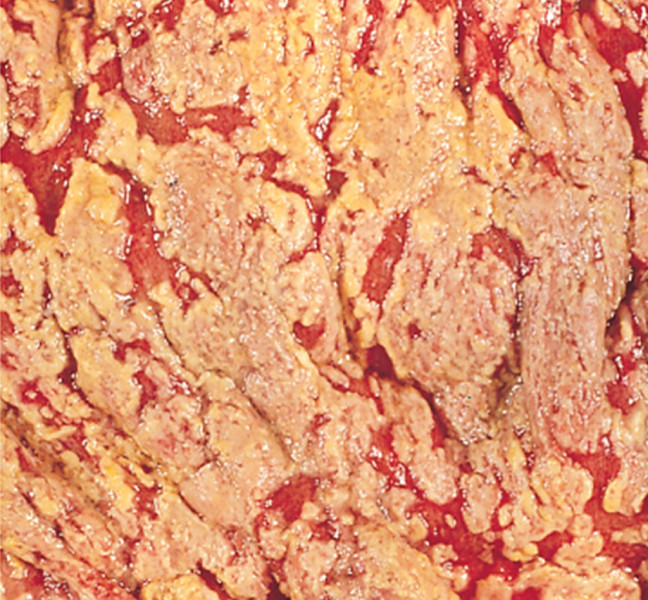
The appendix was swollen, dark red, hemorrhagic, and covered by gray-yellow exudate. Serial cross-sections revealed a distended lumen containing hemorrhagic material and a fecalith, which apparently obstructed the lumen.
|
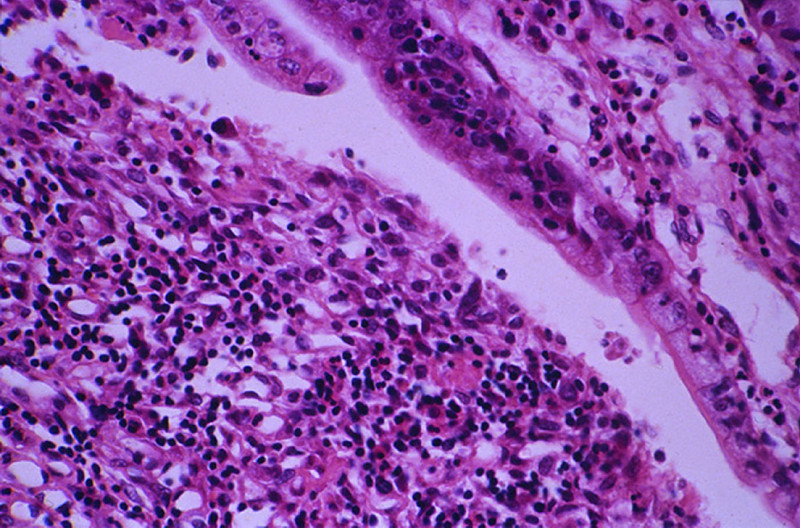
(Summary of Microscopic Findings - click here)
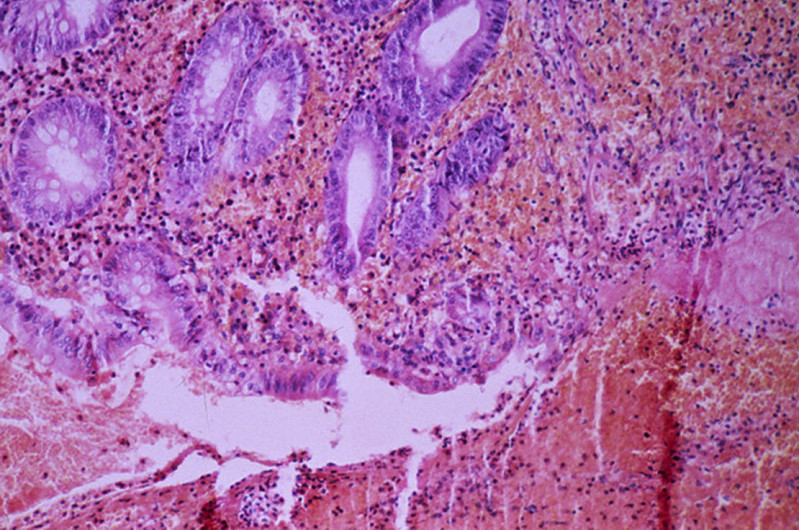
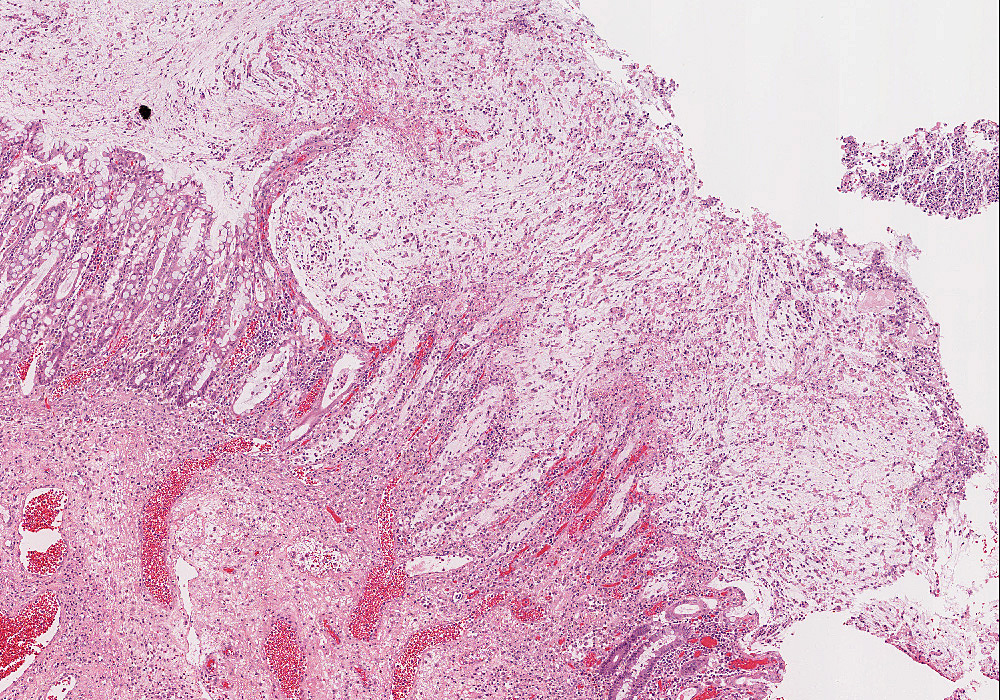
Portions of the mucosa are ulcerated, necrotic and heavily infiltrated with neutrophils. This acute inflammation and necrosis extends throughout the entire thickness of the wall and the serosa. In the lumen of the appendix there is pus and a fecalith.
|
(Review Normal Histology - click here)
Norm No. 8 Appendix
[ImageScope] [WebScope]
The appendix is a tubular organ with a lumen which is lined by mucin secreting columnar epithelium. There is no evidence of acute inflammation. The submucosa and muscle layers are unremarkable. There is no inflammation of the serosa.
|
|
54-1. What is the MOST LIKLEY diagnosis?
- Acute appendicitis
- Chronic appendicitis
- Acute cholecystitis
- Ectopic pregnancy with rupture
ANSWER
54-2. If the anatomic location of this organ were retrocecal, the expected complication would be:
- Retroperitoneal abscess
- Peritonitis
- Infarction
- Sepsis
ANSWER
CASE NUMBER 240
[ImageScope] [WebScope]
Clinical History: This patient was a 54-year-old male who had a long history of peptic ulcer disease. A portion of the stomach was removed. Medical management is more common today.
Image Gallery:
(Summary of Gross Findings - click here)
An endoscopic view shows that the gastric mucosa is somewhat flattened but demonstrates a focal ulcer with smooth edges.
|
(Summary of Microscopic Findings - click here)
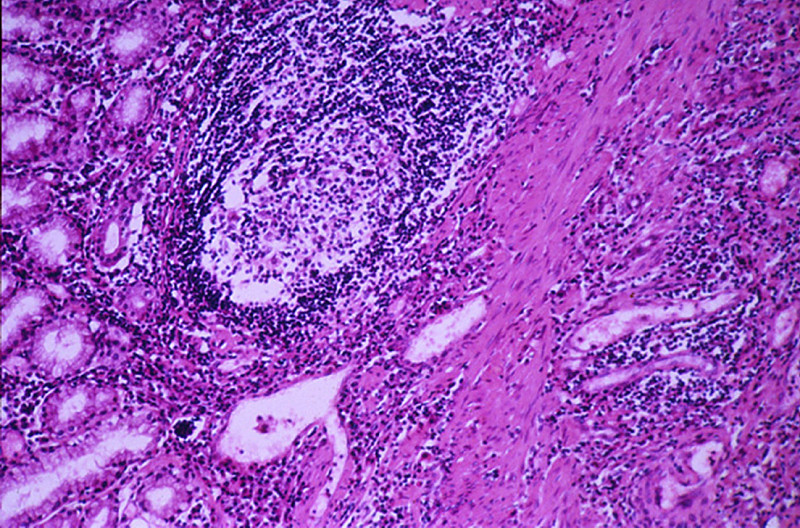
Microscopic sections show a portion of antral/pyloric stomach. A large ulcer and the accompanying response have replaced all layers of the stomach mucosa and wall. Three layers may be distinguished in the bed of the ulcer. The innermost one is composed of necrotic debris and fibrino-purulent exudate in which bacteria and yeast are present. The middle layer is a zone of granulation tissue made up of small vessels and acute and chronic inflammation. The deepest portion of the ulcer is made up of fibrous scar. Some of the arteries in the scar tissue may show sclerosis. The mucosa adjacent to the ulcer shows acute and chronic gastritis.
|
(Review Normal Histology - click here)
Norm No. 16 Stomach, fundus
[ImageScope] [WebScope]
The normal gastric mucosa of the fundus contains superficial fovea arranged in leaf like fronds and deeper gastric glands. The foveolar cells secrete mucin. The gastric glands include mucous cells, parietal cells, chief cells and enteroendocrine cells.
|
240-1. This patient’s lesion is best characterized as:
- Acute gastric ulcer
- Chronic gastric ulcer
- Acute gastric abscess
- Chronic gastric abscess
ANSWER
240-2. As this lesion erodes through the stomach wall, a red granular exudate forms on the serosal surface. The exudate is:
- Serous
- Fibrinous
- Fibrinopurulent
- Purulent
ANSWER
240-3. Should the ulcer penetrate the anterior wall of the stomach, within an hour the patient would have:
- Acute peritonitis
- Chronic peritonitis
- Acute cellulitis
- Chronic abscess
ANSWER
240-4. If the ulcer penetrates the posterior wall of the stomach, within an hour the patient would have
- Acute peritonitis
- Chronic peritonitis
- Acute cellulitis
- Chronic abscess
ANSWER
Microbiology Case Descriptions
Micro Case 5
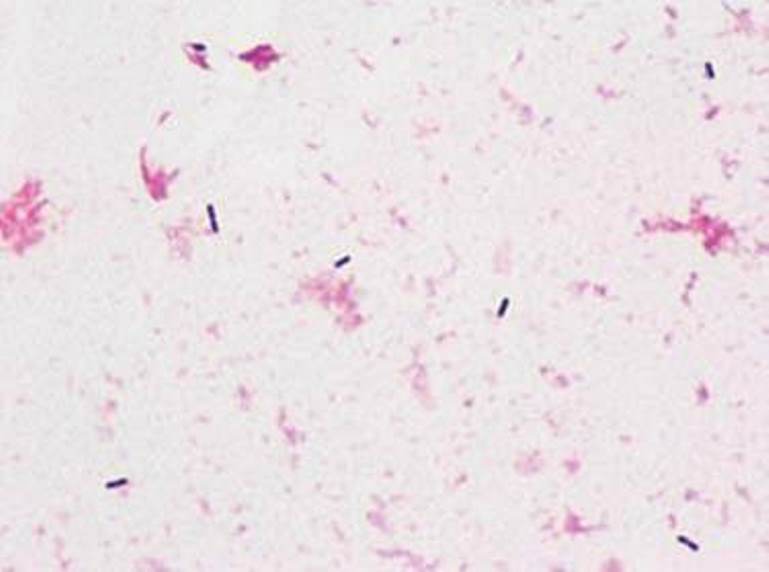
Clinical history: A 33-year-old female dairy farmer develops a severe headache and neck stiffness. On physical examination, her temperature is 38.2°C. She has no papilledema. A lumbar puncture is performed, and a Gram stain of the CSF obtained shows many short, gram-positive rods.
Image Gallery:
m5-1. Based on the clinical findings presented, what is the most likely causative agent in the case above?
ANSWER
m5-2. A sputum gram stain of an elderly person with cough and fever shows gram positive cocci in pairs. What is the most likely organism?
- Haemophilus influenzae
- Streptococcus pyogenes
- Enterobacter species
- Streptococcus pneumoniae
ANSWER
Micro Case 9
Clinical history: A 52-year-old homeless, alcoholic man had a fever and a cough productive of thick sputum that worsened over several days. His temperature is 38.2°C. Diffuse crackles are heard at the right lung base. Laboratory studies are as follows:
- hemoglobin: 13.3 g/dL
- hematocrit: 40%
- platelet count: 291,8000/mm3
- WBC count: 13,240/mm3 with 71 segmented neutrophils, 7% bands, 16% lymphocytes, and 6% monocytes.
Image Gallery

m9-1. Based on these clinical findings, what is the likely causative agent?
ANSWER
m9-2. An 18-year-old Duke freshman presented to student health with severe headache, fever, and disorientation. A lumbar tap was performed with the following results:
- cell count: 300 with 100% PMN
- glucose: 10 mg/dl
- protein: 100 mg/dl.
The gram stain of the spinal fluid revealed numerous PMNs with intracellular gram-negative diplococci. What is the most likely organism?
- Streptococcus pneumoniae
- Moraxella catarrhalis
- Haemophilus influenza
- Neisseria meningitides
ANSWER
Micro Case 10
Clinical history: A 66-year-old man incurs extensive thermal burns to his skin and undergoes skin grafting procedures in the surgical intensive care unit. Two weeks later, he has increasing respiratory distress. Laboratory studies show hemoglobin of 13.1 g/dL, hematocrit 39.2%, platelet count 222,200/mm3, and WBC count 4520/mm3 with 15% monocytes. A chest radiograph shows extensive bilateral infiltrates with patchy areas of consolidation.
Image Gallery:
(Summary of Gross and Lab Findings - click here)
A photograph of burn patient is shown. There is a thick purulent exudate on the skin surface. Cultures of the wound on MacConkey and sheep blood agar (SBA) showed aerobic, lactose-negative, Gram-negative bacterium.
|
m10-1. Based on these clinical findings, what is the likely causative agent?
ANSWER
m10-2. A sputum specimen from a cystic fibrosis patient grew Gram negative rods on sheep blood agar and MacConkey’s agar. The organism was oxidase positive. What is the most likely organism?
- Streptococcus pneumoniae
- Klebsiella pneumoniae
- Pseudomonas aeruginosa
- Enterococcus species
ANSWER
Micro Case 12 (UMich Slide 017)
[ImageScope] [WebScope]
Clinical history: A 45-year-old woman is being treated in the hospital for pneumonia complicated by septicemia. She has required multiple antibiotics and was intubated and mechanically ventilated earlier in the course. On day 20 of hospitalization, she has abdominal distention. Bowel sounds are absent, and abdominal radiograph shows dilated loops of small bowel suggestive of ileus. She has a low volume of bloody stool.
Image Gallery
m12-1. Based on these clinical findings, what is the likely causative agent?
ANSWER
m12-2. Which of the following are appropriate specimen samples for anaerobe culturing:
- blood, spinal fluid, abscess aspirate
- deep tissue biopsy, sputum, blood
- cerebrospinal fluid, tissue and debridement from decubitus ulcer, bile
- tissue swabs, blood, urine
ANSWER
Micro Case 13
Clinical history: A 25-year-old man is involved in an accident in which he is ejected from the vehicle. He sustains a compound fracture of the left humerus and undergoes open reduction with internal fixation of the humeral fracture. Several days later, he has marked swelling of the left arm and crepitus.
Image Gallery
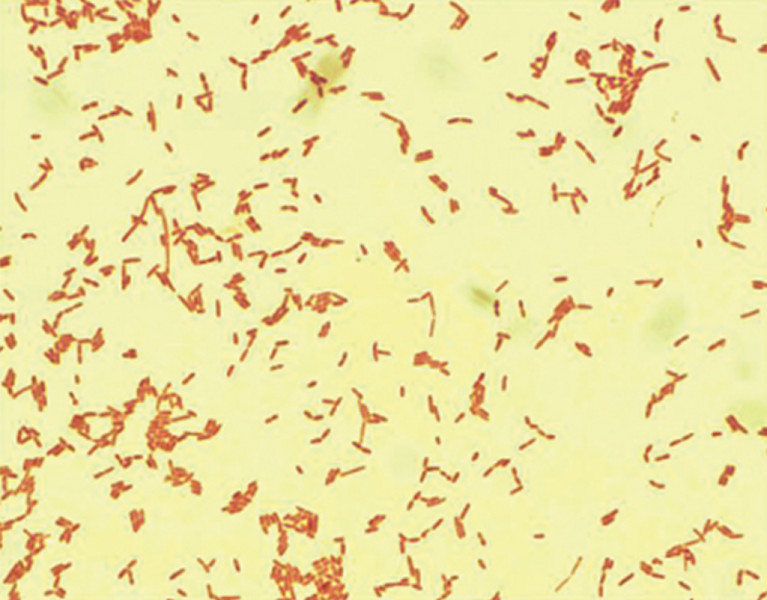
(Summary of Gross and Lab Findings - click here)
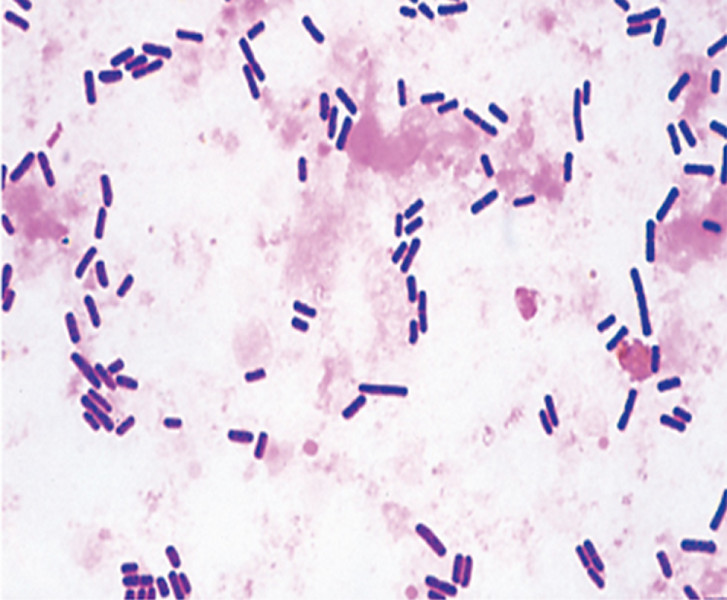
On the arms, there is marked swelling and tissue destruction with black discoloration. Boxcar shaped gram positive rods are seen in the gangrenous tissue. The organism requires anaerobic culture conditions and egg yolk agar for growth.
|
m13-1. In a similar case, a middle aged woman with type 2 diabetes presents to the emergency room with a very painful right lower leg. She has a wound on that extremity and stated that she stumbled on a fallen tree limb in her yard. You observe that her lower leg is discolored and swollen with several areas of crepitus. The abscess fluid was sent to the microbiology laboratory for aerobic and anaerobic culture. The organism grew best on anaerobic cultures and was lecithinase positive. Gram stain shows gram positive rods and the organism show anaerobic growth on egg yolk agar. What is the most likely organism?
- Fusobacterium nucleatum
- Bacteroides fragilis
- Clostridium perfringens
- Peptostreptococcus spp.
ANSWER
Review Items
THROMBOSIS, HEMOSTASIS, EDEMA, and SHOCK
Key Vocabulary Terms
HEMOSTASIS and THROMBOSIS LEARNING OBJECTIVES
Absolutely critical information you must know to practice medicine is in bold font.
Important information that will be needed for routine patient care is in regular font.
Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics.
- Outline the process of normal hemostasis; role and interaction of each element
- Intrinsic pathway
- extrinsic pathway
- final common pathway
- fibrin formation and fibrinolysis
- protein C/protein S pathway
- role of platelets
- role of vascular integrity
- events in dissolution of a thrombus
- Compare acute and chronic hemorrhage in terms of:
- common causes
- clinical manifestations
- compensatory mechanisms
- Describe thrombi in terms of:
- types of thrombotic material
- factors conditioning the development of thrombi
- possible fate of thrombi
- Distinguish between venous thrombi and arterial thrombi on the basis of:
- etiologic and precipitating factors
- common sites of occurrence
- type and size of vessel involved
- morphologic appearance
- organs commonly involved
- local and distant effects
- fate of lesions and prognosis
- clinical and laboratory features
- Compare the following types of emboli in terms of morphologic features, precipitating factors, common sites, organs involved, type of vessel, complications, clinical presentation
- Compare and contrast arterial and venous infarcts on the basis of:
- location
- pathogenesis
- morphology
- clinical manifestations
- Describe the morphologic appearance and natural history of infarcts of:
- heart
- lung
- bowel
- kidney
- spleen
- brain
- Define, state the significance of, and identify on a peripheral blood smear:
- Discuss thrombocytopoiesis in terms of:
- morphology of megakaryocytes
- fate of megakaryocytes
- life span of platelets
- factors which influence thrombocytopoiesis
- abnormal morphologic forms of platelets and megakaryocytes
- Discuss thrombocytopenia in terms of:
- differential diagnosis
- clinical features
- bone marrow morphology and
- laboratory features
- Compare and contrast bleeding due to:
- vascular defect (localized or generalized)
- platelet defect
- coagulation defect
- Discuss thrombocytosis in terms of diagnosis and differential diagnosis
- Outline the process for stepwise evaluation of a:
- bleeding patient
- patient with suspected platelet disorder
- patient with suspected hypercoagulability
- Compare and contrast:
- List and discuss the laboratory diagnostic procedures for patients with:
- bleeding disorders
- thrombotic disorders
- Compare and contrast bleeding disorders due to:
- Describe the mechanism(s) by which the following drugs affect hemostasis:
- aspirin
- coumadin (warfarin)
- heparin
EDEMA AND SHOCK LEARNING OBJECTIVES
Absolutely critical information you must know to practice medicine is in bold font.
Important information that will be needed for routine patient care is in regular font.
Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics.
- Compare and contrast the following types of shock:
- List the morphologic changes and functional effects of shock on:
- lungs
- kidneys
- adrenals
- brain
- gastrointestinal tract
- Compare and contrast
- Compare:
- Describe chronic passive congestion in:
- lung
- liver
- kidneys
- spleen
- Discuss the pathogenesis of edema, giving examples associated with:
- altered plasma oncotic pressure
- inflammation
- venous obstruction/stasis
- lymphatic obstruction
- Compare the consequences of edema in:
- subcutaneous tissue
- lungs
- brain
- kidneys
HEMODYNAMICS AND ARTERIOSCLEROSIS
Key Vocabulary Terms
HEMODYNAMICS and ARTERIOSCLEROSIS LEARNING OBJECTIVES
Absolutely critical information you must know to practice medicine is in bold font.
Important information that will be needed for routine patient care is in regular font.
Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics.
- Discuss mechanisms of blood pressure regulation, including:
- cardiac influences
- neural factors
- hormonal factors
- vasoactive agents
- renin-angiotensin system
- Compare and contrast clinical and pathologic features of the following types of hypertension:
- Discuss the morphologic effects of hypertension on:
- heart
- brain
- kidneys
- placenta
- Discuss the clinical and pathologic features of the following vascular diseases :
- Discuss the clinical and pathologic features of the following forms of vasculitis:
- Compare and contrast the clinical and pathologic features of the following disorders:
- Compare and contrast thoracic and abdominal aortic aneurysms on the basis of:
- etiologic factors
- incidence
- complications
- Discuss the effects of the following on the pathogenesis and prevalence of atherosclerosis:
- age
- sex
- geographic location
- risk factors
- Outline the development of the atherosclerotic lesion with respect to:
- pathogenic mechanisms
- morphology
- clinical manifestations
- complications
- Compare and contrast the clinical and pathologic features of:
|