Pathology Cases for Week 7
Pathology Case Descriptions
CASE NUMBER 92
[ImageScope] [WebScope]
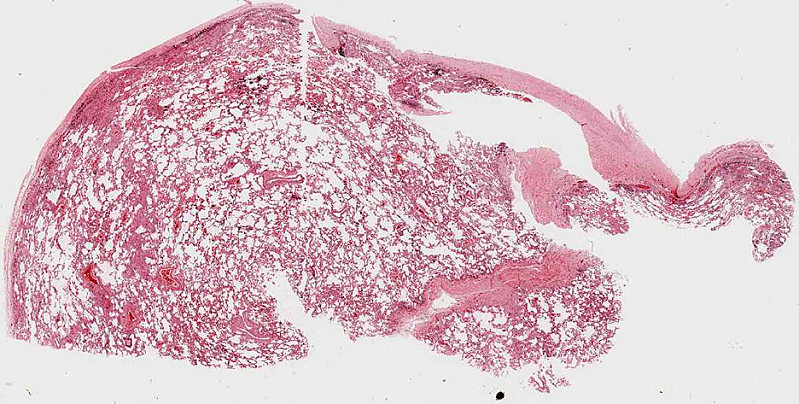
Clinical History: A 65 year old male had smoked for many years. He complained about increasing dyspnea over the last 10 years. The dyspnea had suddenly increased and the patient was admitted with signs of heart failure. He died one week after admission from an acute brain infarct.
Image Gallery:
(Summary of Gross Findings - click here)
The lungs were very large and upon palpation there was marked crepitation.
|
(Summary of Microscopic Findings - click here)
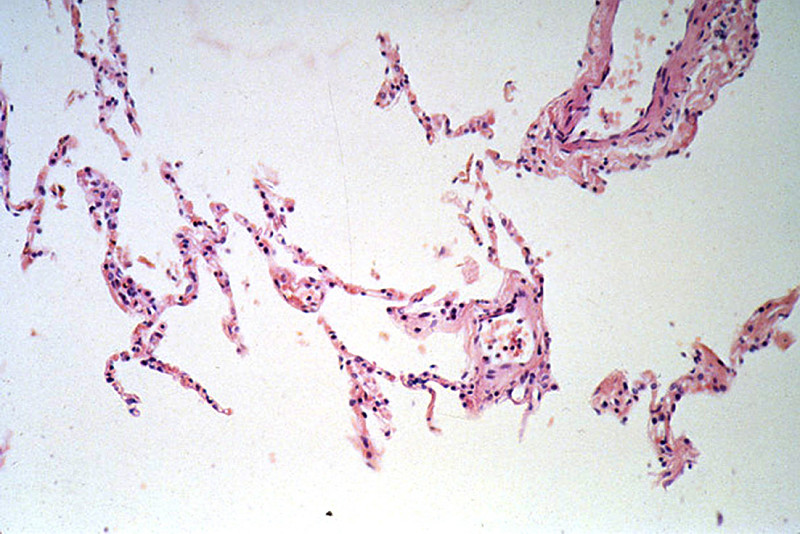
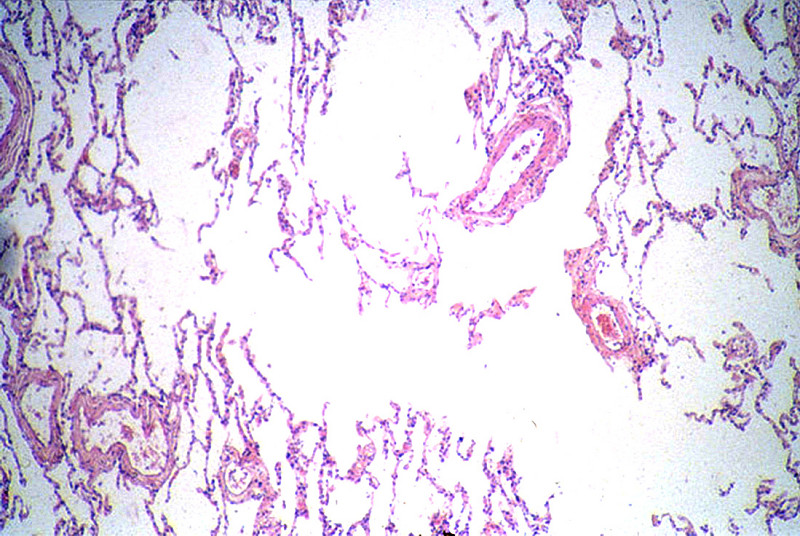
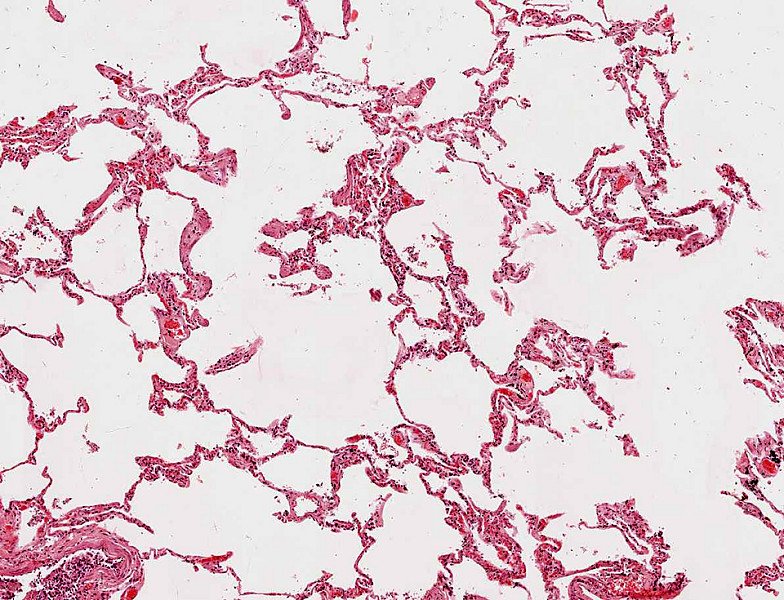
The alveolar spaces are distended and the alveolar septa are thickened by fibrous tissue. Numerous "free floating" alveolar septa are present, recognizable as pieces at alveolar wall not connected at either end to adjacent septa.
|
(Review Normal Histology - click here)
Norm No. 24 Lung
[ImageScope] [WebScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
|
92-1. What is the most likely diagnosis?
- Lung abscesses
- Panacinar emphysema
- Asbestosis
- Centrilobular emphysema
ANSWER
92-2. What factor contributed most to this patient’s disease?
- Living in South Carolina
- Genetics
- Cigarette smoking
- Alcohol consumption
ANSWER
CASE NUMBER 233
[ImageScope] [WebScope]
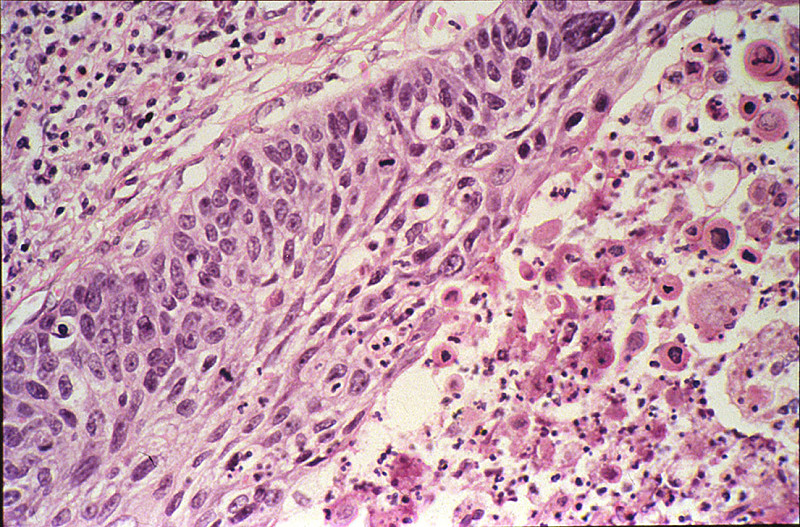
Clinical History: This 23-year-old white female was found to have a cervical lesion three months previous to this admission. A biopsy revealed carcinoma of the cervix. The uterus was removed. Preoperative radiation therapy is common today.
Image Gallery:
(Summary of Gross Findings - click here)
The entire external cervix showed a large, gray-pink, fungating lesion, 5.5 cm in size. It extended into the internal cervical canal and also involved one of the obturator lymph nodes.
|
(Summary of Microscopic Findings - click here)
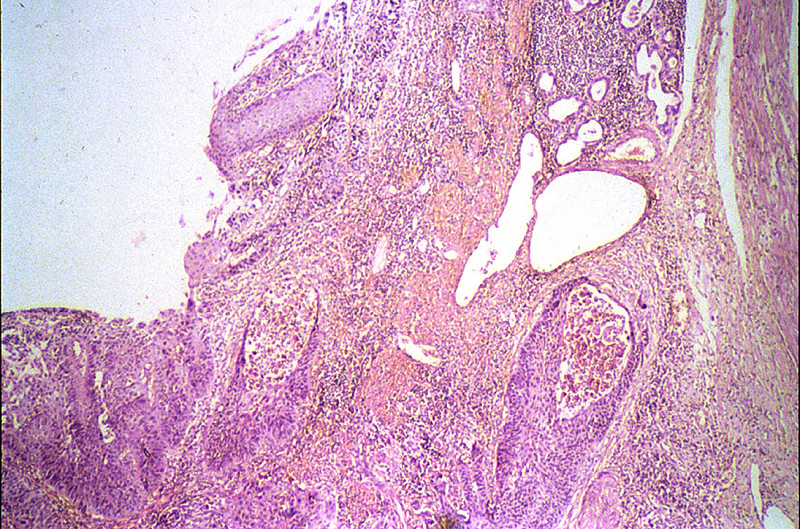
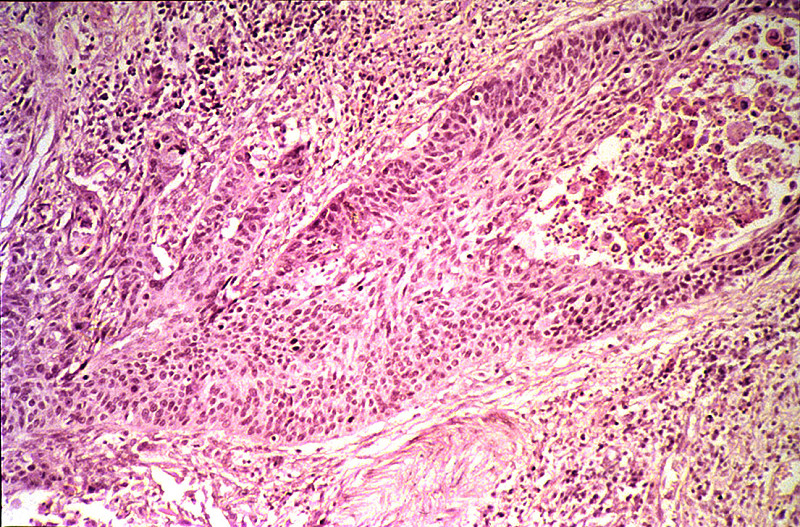
The external cervix shows fibrosis and acute and chronic inflammatory infiltration. A portion of the cervical mucosa is infiltrated with squamous cell carcinoma. The tumor cells are pleomorphic and bizarre and frequently form giant cells. Strands and nests of the tumor cells are seen in the cervical stroma. Marked acute and chronic inflammation is present in association with the tumor.
|
(Review Normal Histology - click here)
Slide 249 (cervix, H&E) WebScope ImageScope
UCSF slide 405 (cervix, trichrome) WebScope ImageScope
The uterine cervix shown in slide 249 is continuous with both the body of the uterus and the upper portion of the vagina. Note that the wall has considerable smooth muscle and much dense connective tissue. Note also the number of collagen fibers in the stroma.
The mucosa is lined by a tall columnar mucus-secreting epithelium in its uterine portion, but note the abrupt change to stratified squamous epithelium at its vaginal face. This stratocolumnar junction which should be readily identifiable in both slide 249 [example] and UCSF slide 405 [example] is frequently the site of pre-neoplastic and neoplastic (cervical cancer) changes. The mucosa is thrown into deep irregular folds known as plicae palmitae (palmate folds). During the majority of the uterine cycle these glands secrete a highly viscous mucus forming a barrier to microorganisms, while at mid-cycle (ovulation) the mucus becomes more hydrated, which facilitates sperm entry. Blockage of the openings of the cervical mucosal glands frequently results in the accumulation of secretory products within the glands, leading to the formation of dilated Nabothian cysts which may be seen in USCF slide 304 [example]. These cysts are generally benign; however, they can become clinically relevant should they become enlarged enough to cause obstruction of the cervical canal.
|
What is the MOST LIKELY diagnosis?
ANSWER
233-1. Which of the following statements about this tumor is/are true?
- It may present at any age of life from second decade onwards
- Related to HPV infection
- Fungating tumor in the cervix
- 95% of squamous cell carcinomas are large cell
- ALL of the above
- NONE of the above
ANSWER
CASE NUMBER 129
[ImageScope] [WebScope]
Clinical History: A 70-year-old white male had an insidious onset of dysphagia of six months duration. X-ray revealed a filling defect and stenosis in the lower esophagus. An esophageal resection was performed.
Image Gallery:
(Summary of Gross Findings - click here)
The resected esophagus contained a firm, raised, pink-gray, friable and necrotic 3.5 x 4.5 cm tumor mass, completely encircling the esophagus and producing a marked stenosis.
|
(Summary of Microscopic Findings - click here)
At one end of the section the squamous epithelium of the esophagus shows marked atypia, pleomorphism and loss of polarity, but no submucosal invasion. These changes represent carcinoma in situ. By following the mucosal lining, one comes upon an area where the cords and nests of poorly differentiated squamous cells are seen to invade the mucosa and submucosa reaching the muscular layer. At one margin of the section the tumor cells are better differentiated with production of keratin and formation of so-called epithelial pearls. Associated with the tumor are marked fibrous proliferation and intense chronic inflammatory infiltration in the stroma. The tumor invades into, but not through the muscularis externa.
|
(Review Normal Histology - click here)
Slide UCSF 226 (esophagus, H&E) WebScope ImageScope
Slide UMich 126 40x (trachea & esophagus, H&E) WebScope ImageScope
Slide UMich 153 20x (esophagus, H&E) WebScope ImageScope
Slide UMich 155 40x (gastro-esophageal junct, H&E) WebScope ImageScope
For the purpose of histological descriptions, the esophagus is subdivided into upper (entirely skeletal muscle in the muscularis externa), middle (mixed smooth and skeletal muscle) and lower (entirely smooth muscle) portions. Slide UCSF 226 is from the upper 1/3; slides 126 and 153 are from the middle 1/3; and slide 155 is from the lower 1/3 (at the esophageal-cardiac junction). The esophageal epithelium [example] is the non-keratinized stratified squamous type and is supported by a connective tissue lamina propria. Note the presence of isolated lymphoid nodules [example] and scattered leukocytes in the lamina propria. A rather thick layer of longitudinally arranged smooth muscle fibers form the muscularis mucosae [example]. The connective tissue of the submucosa consists of mostly collagenous fibers with some elastic fibers and varying amounts of fat as well as submucosal sero-mucous glands which can be readily observed in both slide 126 [example] and slide 153 [example] (those in slide 155 are not very well preserved).
In the upper esophagus, as shown in Slide UCSF 226, the muscularis externa consists of both inner and outer layers of skeletal muscle only. In the middle esophagus, the muscularis externa contains a mixture of skeletal and smooth muscle as seen in slide 126 [example], whereas in the lower esophagus only smooth muscle is found as seen in slide 155 [example]. Present in all regions of the esophagus (upper, mid, and lower) is the myenteric (Auerbach’s) plexus [example] between the two layers of the muscularis externa (W pg 267, 14.3). For most of its extent, the esophagus is retroperitoneal, so its outermost layer consists of a connective tissue adventitia which merges with the adjacent connective tissue associated with nearby structures (such as the trachea as shown in slide 126). Below the diaphragm, however, the esophagus is suspended within abdominal cavity and is therefore covered by a connective tissue serosa as shown in slide 155.
|
What is the MOST LIKELY diagnosis?
ANSWER
129-1. What is the least important contributory risk factor for this neoplasm?
- Alcohol and tobacco abuse
- Barrett esophagus
- Human papilloma virus
- Fungi, nitrates, nitrosamines in food
ANSWER
129-2. The most important risk factor for adenocarcinoma of the esophagus is:
- Alcohol and tobacco abuse
- Barrett esophagus
- Human papilloma virus
- Fungi, nitrates, nitrosamines in food
ANSWER
CASE NUMBER 60 [ImageScope] [WebScope]
Clinical history: This histologic section was prepared from the lung of a 72-year-old man, who was a retired shipyard worker with a history of smoking and mild dyspnea and died of a myocardial infarct.
Image Gallery (slide specimen and images courtesy of the University of Michigan):
(Summary of Gross Findings - click here)
At autopsy, the pleural surfaces of both lungs were fibrotic. The cut surfaces of the lungs manifested diffuse fibrosis with extensive 'honeycombing.' The hilar lymph nodes were not enlarged.
|
(Summary of Microscopic Findings - click here)
Many of the alveolar walls contain more nuclei than usual and there are detached fragments of alveolar septa. Small deposits of anthracotic pigment are also evident. Many of the alveolar septa are thickened by fibrosis. Within these areas of fibrosis are golden brown beaded or 'knobby' structures.
|
(Review Normal Histology - click here)
Norm No. 24 Lung
[ImageScope] [WebScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
|
-
The fibrotic alveolar walls represent a nonspecific reaction to injury that is a common pathologic feature in many lung diseases. In this case, the golden brown bodies represent the etiologic agent. What are these bodies?
ANSWER
-
How did the fibrosis come about?
ANSWER
-
For what other pulmonary disorders or complications was this individual at increased risk?
ANSWER
CASE NUMBER 98
[ImageScope] [WebScope]
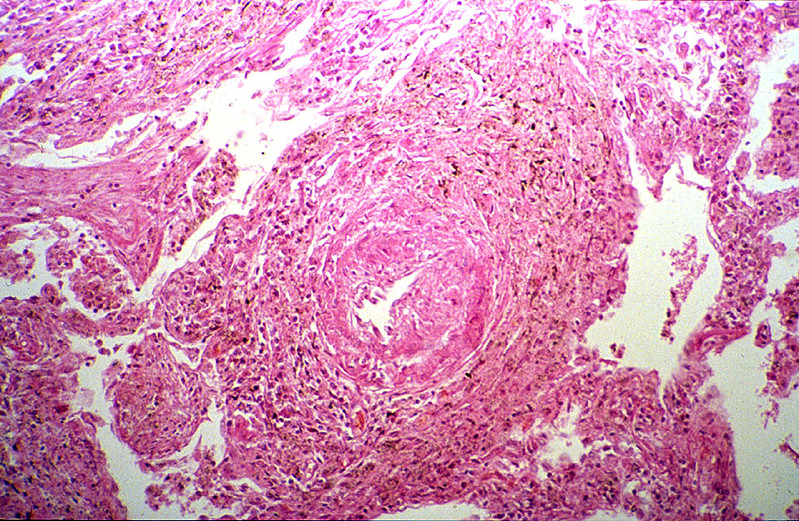
Clinical History: This 70-year-old man worked in a rock quarry as a crusher for 18 years. Six months prior to death he began to have dyspnea, orthopnea, paroxysmal nocturnal dyspnea and ankle edema. He was admitted for congestive heart failure and died suddenly with massive pulmonary embolism.
Image Gallery:
(Summary of Gross and Lab Findings - click here)
Both lungs were heavy, 900 grams for the left lung and 1120 grams for the right one. The lung was slate gray and firm.
|
(Summary of Microscopic Findings - click here)
In the left upper part of the section the characteristic lesions of silicosis are seen. There are masses of fibrous tissue which form concentric lamination around the blood vessels, and stellate scars when the fibrosis extends to the adjacent alveolar septa. A large amount of coal-black pigment and small crystals are found in the macrophages and the scar tissue. These crystals are best seen under polarized light. In advanced lesion the fibrous nodules become confluent as seen in the lower right part of this section. Notice the presence of arteriosclerosis and organizing thrombi in the pulmonary arteries and chronic inflammation of bronchi.
|
(Review Normal Histology - click here)
Norm No. 24 Lung
[ImageScope] [WebScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
|
98-1. Which of the following is most frequently affected in this disease?
- Pleura
- Lower lobes of lungs
- Upper lobes of lungs
- Pulmonary arteries
ANSWER
98-2. Patients with this disease are at increased risk for development of:
- Pneumococcal pneumonia
- Histoplasmosis
- Tuberculosis
- Bronchogenic carcinoma
ANSWER
98-3. The most likely diagnosis as depicted by these images and based on the history is:
- Asbestosis
- Silicosis
- Anthracosis
- Berylliosis
- Siderosis
ANSWER
98-4. Which of the following statements is TRUE?
- Fibrotic nodules with concentric layers of hyalinized collagen is typical of anthracosis
- Asbestosis is marked by localized pleural plaques
- Silicotic nodules may undergo central cavitation
- Progressive massive fibrosis is a common complication of exposure to asbestos
- Coal workers’ pneumoconiosis is associated with increased susceptibility to tuberculosis
ANSWER
ENVIRONMENTAL PATHOLOGY Review Items
Key Vocabulary Terms (click here to search any additional terms on Stedman's Online Medical Dictionary)
LEARNING OBJECTIVES
Absolutely critical information you must know to practice medicine is in bold font.
Important information that will be needed for routine patient care is in regular font.
Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
- Discuss the following in terms of role in indoor vs. outdoor air pollution:
- List the various substances found in cigarette smoke and their health effects.
- Discuss the effects and clinical significance of:
- active tobacco smoke
- passive (sidestream) tobacco smoke
- smokeless tobacco
- Outline the basic pathogenesis of pneumoconioses.
- Compare and contrast the following pneumoconiosis in terms of types of occupational exposure, pathogenesis and clinical course
- Compare coal workers' pneumoconiosis with simple asymptomatic anthracosis.
- Discuss Caplan syndrome in relation to coal workers' pneumoconiosis, asbestosis, and silicosis.
- Describe the ways in which the following factors influence chemical injuries:
|
- physical properties of chemical
|
|
|
|
- nutritional status of patient
|
|
|
|
|
- Describe the ways in which the following factors influence chemical injuries:
|
|
|
|
|
|
|
|
|
|
|
|
|
- organochlorine insecticides
|
|
- organophosphate insecticides
|
- Discuss ethanol in terms of:
- effects ethanol on society
- blood alcohol levels and their effects
- metabolism and systemic effects of:
- acute alcohol ingestion
- chronic ethanol abuse
- Discuss the following:
|