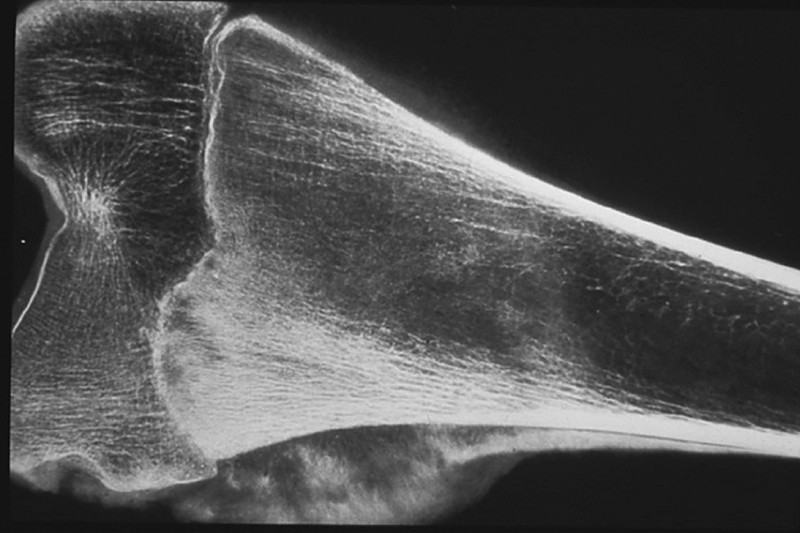
Clinical History: A 13-year-old male had an enlarging mass in the left thigh for 1 1/2 months. It was not associated with pain or tenderness. The X-ray revealed a large tumor extending around the entire shaft and lower 1/3 or the left femur. Amputation was performed after biopsy. Limb salvage surgery is commonly performed today.
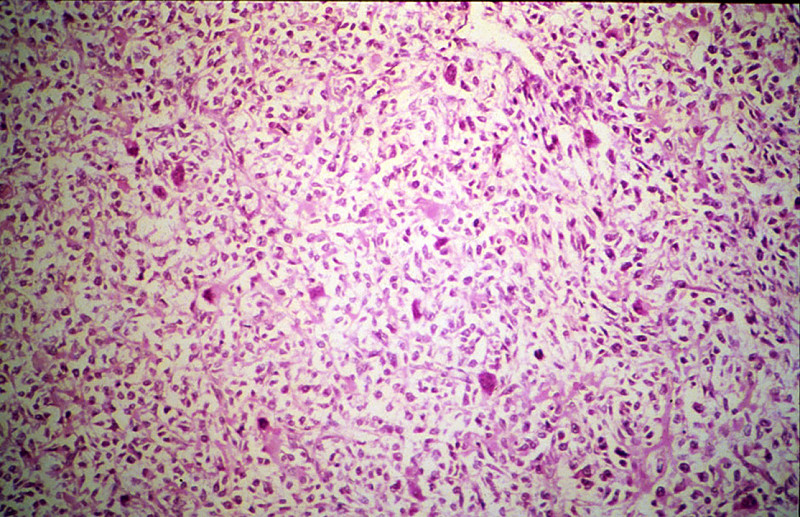
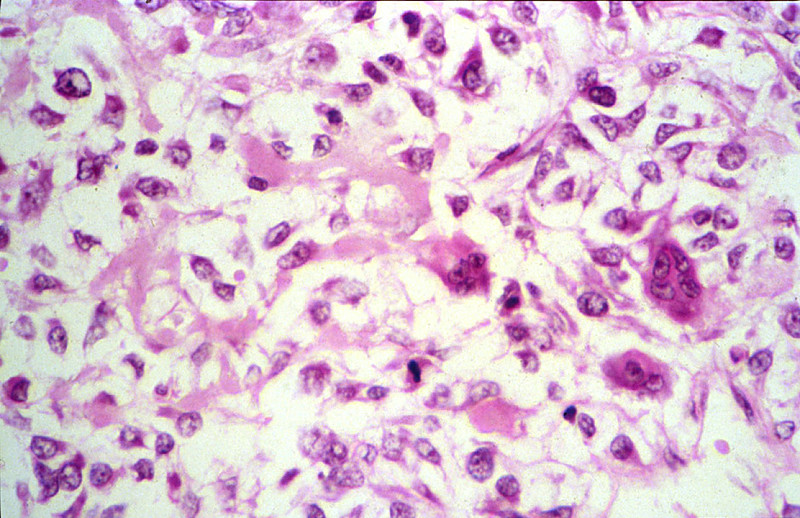
The tumor is composed of sheaths of loosely packed fibroblastic and osteoblastic cells, which have large hyperchromatic nuclei and scanty eosinophilic cytoplasm. In the intercellular spaces of the tumor there is deposition of pink homogeneous osteoid tissue which frequently transforms into irregular, bony trabeculae. New periosteal bone formation may be seen in the section.
Webslide 0301, developing finger, long. sect.
[ImageScope]
[WebScope]
The bones shown in Webslide 301 (distal end of a metacarpal, and the 1st, 2nd, and part of the 3rd phalangeals) are still undergoing the process of endochondral ossification, but there are many general features of long bones that can be appreciated. The shaft of each bone (the diaphysis) consists of a rigid cylinder of compact bone (example) surrounding a hollow marrow cavity (example). Within the marrow cavity are hematopoietic cells and some adipocytes amongst spicules of trabeculated, or spongy, bone. As most long bones mature, the hematopoietic cells are replaced by the adipocytes and the marrow transitions from being 'red' (hematopoietic) to 'yellow' (fatty).
Outside of the cylinder of compact bone is a connective tissue sheath known as the periosteum. The periosteum is further subdivided into an inner, cellular periosteum (close to the bone), which is less dense in nature and made up of fibroblasts and osteoprogenitor cells and an outer, fibrous periosteum made up of dense, irregular connective tissue. The periosteum adheres to the bone by way of Sharpey's fibers that extend from the fibrous layer into the compact bone (example).
The articular surfaces at the ends of the bones (the epiphyses) are comprised of hyaline cartilage. Active growth plates (or epiphyseal plates) may be observed at the proximal ends of the phalanges (example) and the distal end of the metacarpal bone (example) whereas the cartilage at the distal ends of the phalanges exhibits much less proliferation (example), which is consistent with the general pattern of growth observed these and other long bones.
050_HISTO_40X, fibula, cross sect.
[ImageScope]
[WebScope]
This is a cross section of a fibula from an adolescent primate and therefore exhibits characteristics of more mature bone. The marrow cavity still contains a great deal of hematopoietic cells and would therefore be considered ‘red’ --however, note that there is a significant amount of adipose tissue that will increase over time. The shaft of the fibula consists of compact bone which is organized into inner (example) and outer (example) circumferential lamella, made up of bone laid down in concentric layers. Sandwiched between the inner and outer lamellae are collections of osteons, or Haversian systems (example). Within the bone, you can see the individual osteocytes within their lacunae and the small canaliculi through which the osteocytes extend processes to communicate with each other. The periosteum is relatively thin and consists primarily of an outer fibrous layer of dense irregular connective tissue. Outside the periosteum are fibers of skeletal muscle associated with the extensor and flexor compartments of the leg.
223-1. This tumor comprises atypical osteoblastic cells that have large hyperchromatic nuclei with nuclear pleomorphism and frequent mitoses, producing new bone matrix (osteoid). The BEST diagnosis is:
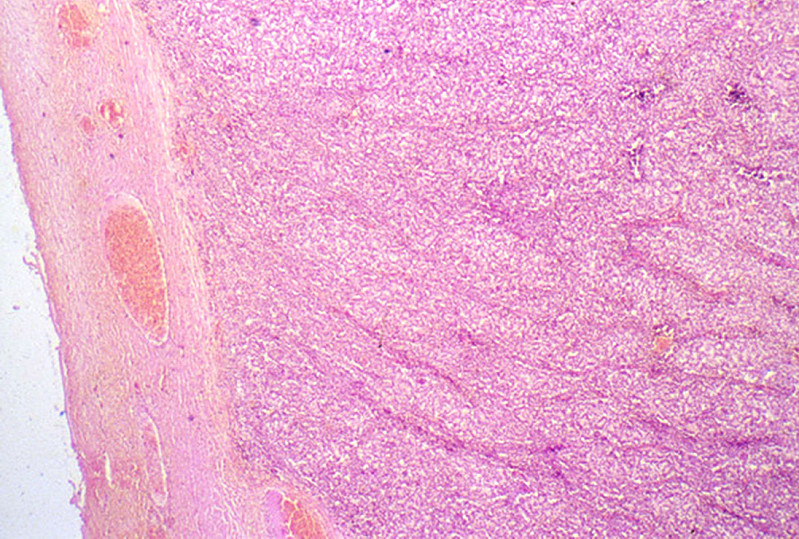
Clinical History: A 30-year-old white female noted intermittent pain and swelling of her knee for 1 1/2 years. She slipped on the stairs and suffered immediate severe pain in the knee. X-ray revealed a tumor which was a large area of decalcification with expansion of tibia, but with thinning of the cortex. Tumors like this are usually treated by curetting. A case that was treated by partial resection of the bone is illustrated.
The tumor is surrounded by a thin rim of cortical bone which is atrophic and shows focal periosteal bone formation. The tumor is composed of many large multinucleated cells and spindle cells resembling fibroblasts. Transitions between these two types of cells may be seen. Many dilated vessels are present in the tumor tissue.
Webslide 0301, developing finger, long. sect.
[ImageScope]
[WebScope]
The bones shown in Webslide 301 (distal end of a metacarpal, and the 1st, 2nd, and part of the 3rd phalangeals) are still undergoing the process of endochondral ossification, but there are many general features of long bones that can be appreciated. The shaft of each bone (the diaphysis) consists of a rigid cylinder of compact bone (example) surrounding a hollow marrow cavity (example). Within the marrow cavity are hematopoietic cells and some adipocytes amongst spicules of trabeculated, or spongy, bone. As most long bones mature, the hematopoietic cells are replaced by the adipocytes and the marrow transitions from being 'red' (hematopoietic) to 'yellow' (fatty).
Outside of the cylinder of compact bone is a connective tissue sheath known as the periosteum. The periosteum is further subdivided into an inner, cellular periosteum (close to the bone), which is less dense in nature and made up of fibroblasts and osteoprogenitor cells and an outer, fibrous periosteum made up of dense, irregular connective tissue. The periosteum adheres to the bone by way of Sharpey's fibers that extend from the fibrous layer into the compact bone (example).
The articular surfaces at the ends of the bones (the epiphyses) are comprised of hyaline cartilage. Active growth plates (or epiphyseal plates) may be observed at the proximal ends of the phalanges (example) and the distal end of the metacarpal bone (example) whereas the cartilage at the distal ends of the phalanges exhibits much less proliferation (example), which is consistent with the general pattern of growth observed these and other long bones.
050_HISTO_40X, fibula, cross sect.
[ImageScope]
[WebScope]
This is a cross section of a fibula from an adolescent primate and therefore exhibits characteristics of more mature bone. The marrow cavity still contains a great deal of hematopoietic cells and would therefore be considered ‘red’ --however, note that there is a significant amount of adipose tissue that will increase over time. The shaft of the fibula consists of compact bone which is organized into inner (example) and outer (example) circumferential lamella, made up of bone laid down in concentric layers. Sandwiched between the inner and outer lamellae are collections of osteons, or Haversian systems (example). Within the bone, you can see the individual osteocytes within their lacunae and the small canaliculi through which the osteocytes extend processes to communicate with each other. The periosteum is relatively thin and consists primarily of an outer fibrous layer of dense irregular connective tissue. Outside the periosteum are fibers of skeletal muscle associated with the extensor and flexor compartments of the leg.
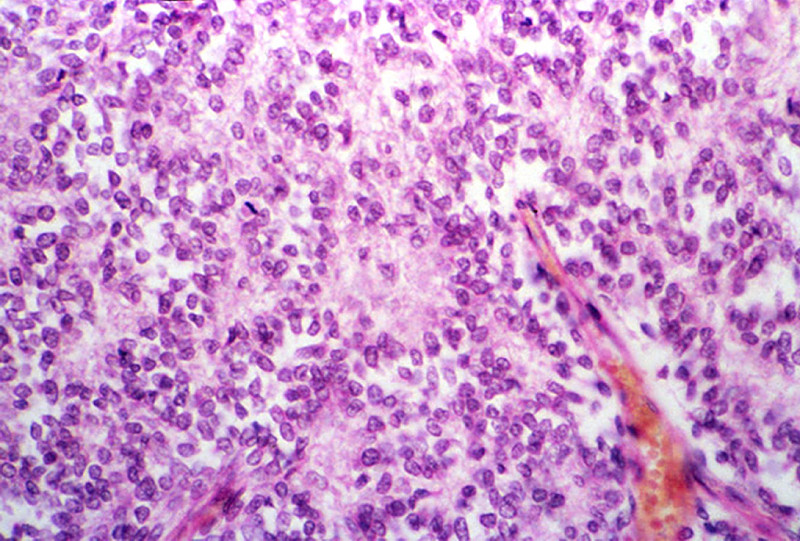
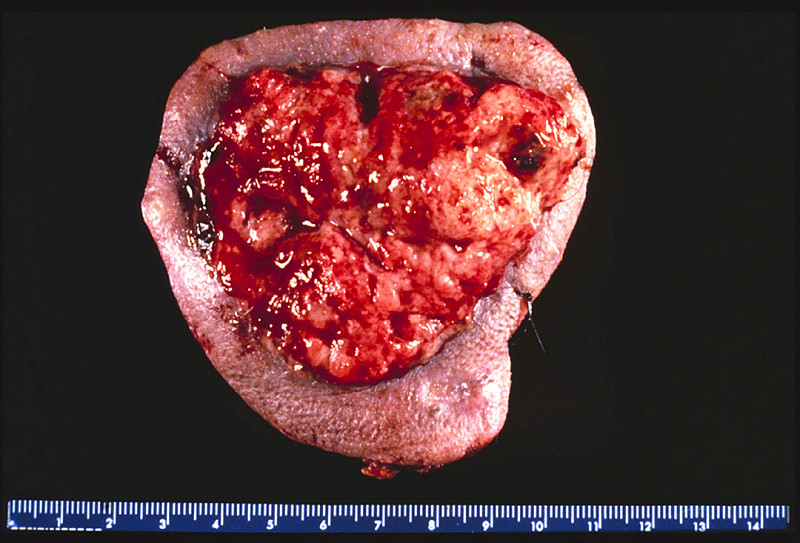
Clinical History: This was a 16-year-old white male who complained of pain and swelling in his hip. He gave a history of having been struck by a baseball four months previously.
The radiograph obtained at presentation shows soft tissue extension of the tumor. Cross section through the resected femoral head shows a soft tan white tumor with focal hemorrhage and necrosis. There is extensive soft tissue invasion.
A striking feature is the monotony of the cells with round to oval vesicular nuclei and poorly defined, scanty eosinophilic cytoplasm. There are a moderate number of mitoses, but tumor giant cells and pleomorphism are conspicuously absent. The tumor cells are arranged around scanty, very vascular, fibrous stroma in a trabecular fashion, sometimes resembling rosette formation. In between these cords the tumor cells seem to line empty spaces. Histologically it is quite difficult to distinguish this tumor from a neuroblastoma.
Webslide 0301, developing finger, long. sect.
[ImageScope]
[WebScope]
The bones shown in Webslide 301 (distal end of a metacarpal, and the 1st, 2nd, and part of the 3rd phalangeals) are still undergoing the process of endochondral ossification, but there are many general features of long bones that can be appreciated. The shaft of each bone (the diaphysis) consists of a rigid cylinder of compact bone (example) surrounding a hollow marrow cavity (example). Within the marrow cavity are hematopoietic cells and some adipocytes amongst spicules of trabeculated, or spongy, bone. As most long bones mature, the hematopoietic cells are replaced by the adipocytes and the marrow transitions from being 'red' (hematopoietic) to 'yellow' (fatty).
Outside of the cylinder of compact bone is a connective tissue sheath known as the periosteum. The periosteum is further subdivided into an inner, cellular periosteum (close to the bone), which is less dense in nature and made up of fibroblasts and osteoprogenitor cells and an outer, fibrous periosteum made up of dense, irregular connective tissue. The periosteum adheres to the bone by way of Sharpey's fibers that extend from the fibrous layer into the compact bone (example).
The articular surfaces at the ends of the bones (the epiphyses) are comprised of hyaline cartilage. Active growth plates (or epiphyseal plates) may be observed at the proximal ends of the phalanges (example) and the distal end of the metacarpal bone (example) whereas the cartilage at the distal ends of the phalanges exhibits much less proliferation (example), which is consistent with the general pattern of growth observed these and other long bones.
050_HISTO_40X, fibula, cross sect.
[ImageScope]
[WebScope]
This is a cross section of a fibula from an adolescent primate and therefore exhibits characteristics of more mature bone. The marrow cavity still contains a great deal of hematopoietic cells and would therefore be considered ‘red’ --however, note that there is a significant amount of adipose tissue that will increase over time. The shaft of the fibula consists of compact bone which is organized into inner (example) and outer (example) circumferential lamella, made up of bone laid down in concentric layers. Sandwiched between the inner and outer lamellae are collections of osteons, or Haversian systems (example). Within the bone, you can see the individual osteocytes within their lacunae and the small canaliculi through which the osteocytes extend processes to communicate with each other. The periosteum is relatively thin and consists primarily of an outer fibrous layer of dense irregular connective tissue. Outside the periosteum are fibers of skeletal muscle associated with the extensor and flexor compartments of the leg.
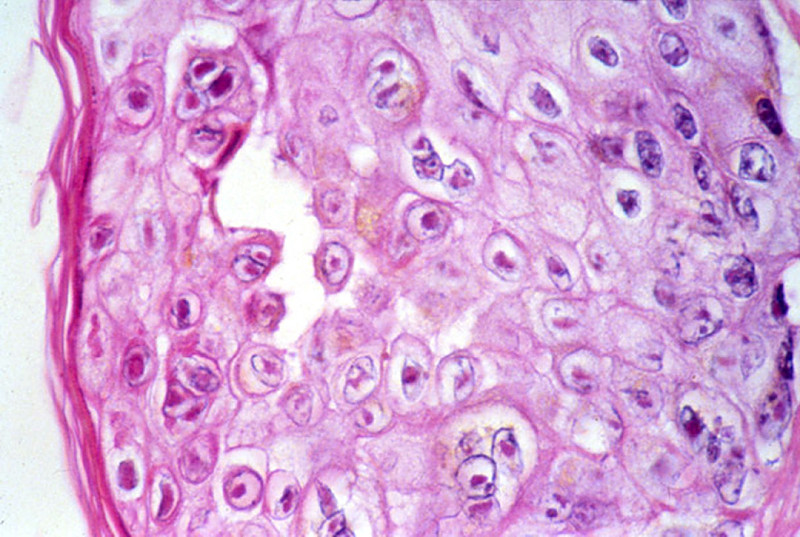
Clinical History: A 62-year-old white male had surgery for renal cell carcinoma. This was followed by chemotherapy. He developed leukopenia, thrombocytopenia and a painful, linear, vesicular rash on his shoulder.
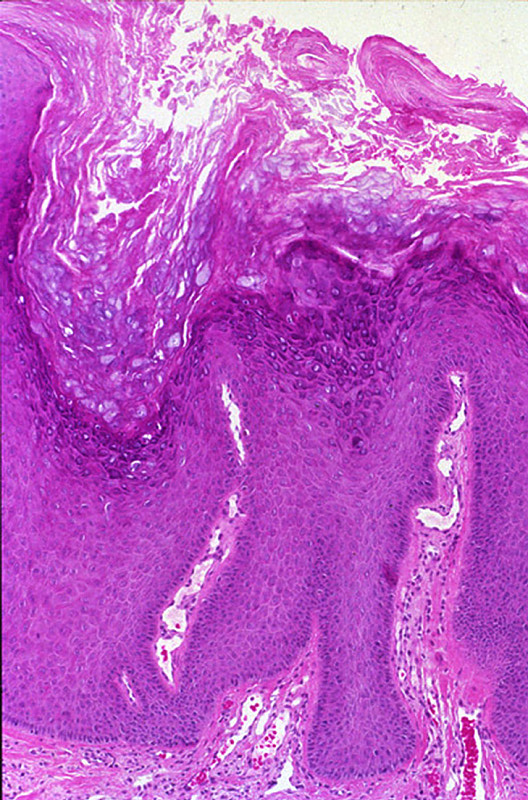
The epidermis shows spongiosis, vesicle formation, necrosis and ulceration. The epidermal cells have degrees of ballooning degeneration. Many intranuclear eosinophilic inclusion bodies are seen in these cells. Many keratinocytes within the vesicle also have multiple nuclei with nuclear "molding" and marginated chromatin. The upper dermis beneath a vesicle shows necrosis with little or no inflammatory reaction.
Webslide 0301, developing finger, long. sect.
[ImageScope]
[WebScope]
The bones shown in Webslide 301 (distal end of a metacarpal, and the 1st, 2nd, and part of the 3rd phalangeals) are still undergoing the process of endochondral ossification, but there are many general features of long bones that can be appreciated. The shaft of each bone (the metaphysis) consists of a rigid cylinder of compact bone (example) surrounding a hollow marrow cavity (example). Within the marrow cavity are hematopoietic cells and some adipocytes amongst spicules of trabeculated, or spongy, bone. As most long bones mature, the hematopoietic cells are replaced by the adipocytes and the marrow transitions from being 'red' (hematopoietic) to 'yellow' (fatty).
Outside of the cylinder of compact bone is a connective tissue sheath known as the periosteum. The periosteum is further subdivided into an inner, cellular periosteum (close to the bone), which is less dense in nature and made up of fibroblasts and osteoprogenitor cells and an outer, fibrous periosteum made up of dense, irregular connective tissue. The periosteum adheres to the bone by way of Sharpey's fibers that extend from the fibrous layer into the compact bone (example).
The articular surfaces at the ends of the bones (the epiphyses) are comprised of hyaline cartilage. Active growth plates (or epiphyseal plates) may be observed at the proximal ends of the phalanges (example) and the distal end of the metacarpal bone (example) whereas the cartilage at the distal ends of the phalanges exhibits much less proliferation (example), which is consistent with the general pattern of growth observed these and other long bones.
050_HISTO_40X, fibula, cross sect.
[ImageScope]
[WebScope]
This is a cross section of a fibula from an adolescent primate and therefore exhibits characteristics of more mature bone. The marrow cavity still contains a great deal of hematopoietic cells and would therefore be considered ‘red’ --however, note that there is a significant amount of adipose tissue that will increase over time. The shaft of the fibula consists of compact bone which is organized into inner (example) and outer (example) circumferential lamella, made up of bone laid down in concentric layers. Sandwiched between the inner and outer lamellae are collections of osteons, or Haversian systems (example). Within the bone, you can see the individual osteocytes within their lacunae and the small canaliculi through which the osteocytes extend processes to communicate with each other. The periosteum is relatively thin and consists primarily of an outer fibrous layer of dense irregular connective tissue. Outside the periosteum are fibers of skeletal muscle associated with the extensor and flexor compartments of the
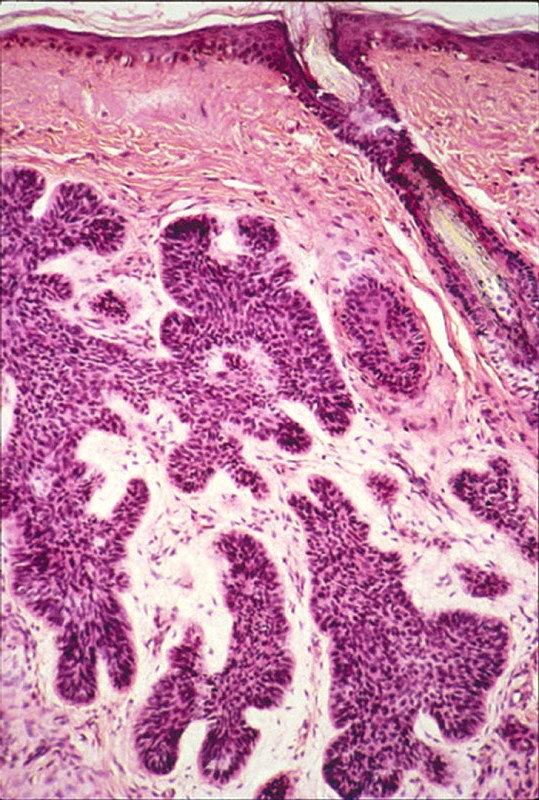
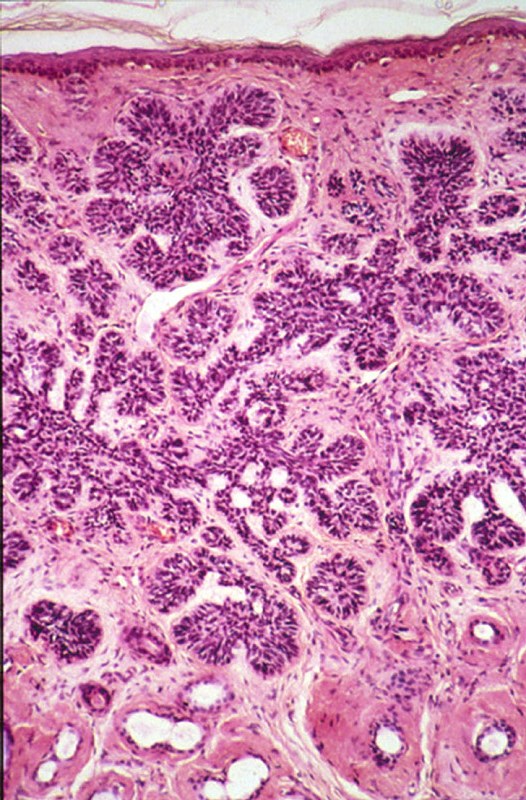
There are nests of darkly staining basophilic cells in the upper dermis with peripheral palisading. There is little cytoplasm, and the cytoplasmic borders are poorly defined. Nuclei are small and are round or oval, and occasional apoptotic bodies are noted. These tumors may arise from the basal cell layer of the epidermis or from dermal appendages. In this particular tumor there is an occasional round mass of keratin which is not usually seen in basal cell carcinomas. Note the loose, myxoid stroma about the tumor cells with some artefactual clefts.
Skin consists of keratinizing stratified squamous epithelium. The keratin layer is eosinophilic. Nuclei are not present. Beneath the keratin layer is a layer of flat epithelial cells with small pyknotic nuclei. Cells are regular and not crowded. These keratinocytes rest upon a layer of basal epithelium and a thin basement membrane. Beneath the epidermis is the dermis which consists of loose connective tissue. Within the dermis are sweat and sebaceous glands. Some slides contain hair follicles. There is no inflammation. The blood vessels are patent and do not contain thromboemboli.
227-1. This skin tumor, which may arise from the basal layer of the epidermis or from dermal appendages is a:
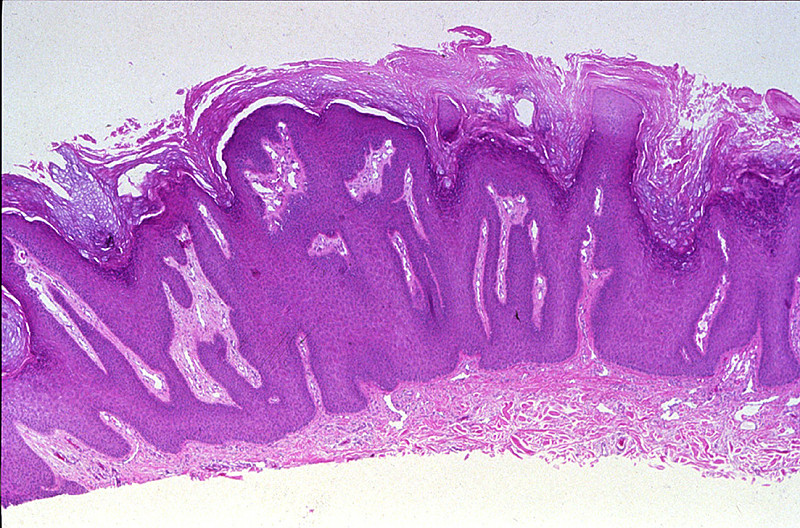
There is marked epidermal hyperplasia with a papillated surface, thickening of the granular layer (hypergranulosis) and cornified layer (hyperkeratosis). Within the granular layer, many of the cells contain large, coarse keratohyalin granules. There are foci of preservation of nuclei in the cornified layer (parakeratosis), especially overlying the tips of the papillae. The vessels in the papillary dermis are dilated.
Skin consists of keratinizing stratified squamous epithelium. The keratin layer is eosinophilic. Nuclei are not present. Beneath the keratin layer is a layer of flat epithelial cells with small pyknotic nuclei. Cells are regular and not crowded. These keratinocytes rest upon a layer of basal epithelium and a thin basement membrane. Beneath the epidermis is the dermis which consists of loose connective tissue. Within the dermis are sweat and sebaceous glands. Some slides contain hair follicles. There is no inflammation. The blood vessels are patent and do not contain thromboemboli.
Clinical history:A 66-year-old man incurs extensive thermal burns to his skin and undergoes skin grafting procedures in the surgical intensive care unit. Two weeks later, he has increasing respiratory distress. Laboratory studies show hemoglobin of 13.1 g/dL, hematocrit 39.2%, platelet count 222,200/mm3, and WBC count 4520/mm3 with 15% monocytes. A chest radiograph shows extensive bilateral infiltrates with patchy areas of consolidation.
A photograph of burn patient is shown. There is a thick purulent exudate on the skin surface. Cultures of the wound on MacConkey and sheep blood agar (SBA) showed aerobic, lactose-negative, Gram-negative bacterium.
m10-1. Based on these clinical findings, what is the likely causative agent?
m10-2. A sputum specimen from a cystic fibrosis patient grew Gram negative rods on sheep blood agar and MacConkey’s agar. The organism was oxidase positive. What is the most likely organism?
Clinical history:A suspicious envelope arrived for sorting at rural post office. The envelope was opened and found to contain white powder. Approximately two days later, the postal worker who handled the letter developed cutaneous boils, which were and 1 to 5 cm in diameter with central necrosis and eschars. He and his wife also developed a mild nonproductive cough with fatigue, myalgia for 72 hours, followed by severe dyspnea, diaphoresis and cyanosis. Temperature of 39.5°C, pulse 105/min, respiration 25/min, and blood pressure 85/45mm Hg. Crackles were heard at the lung bases. A chest xray shows a widened mediastinum and small pleural effusions. WBC count of 13,130/mm3, hemoglobin 13.7g/dL, hematocrit 41.2%, MCV 91 um3, and platelet count 244,000/mm3. Both died despite antibiotic therapy. Several cattle, horses, and sheep on the postal worker's farm also died.
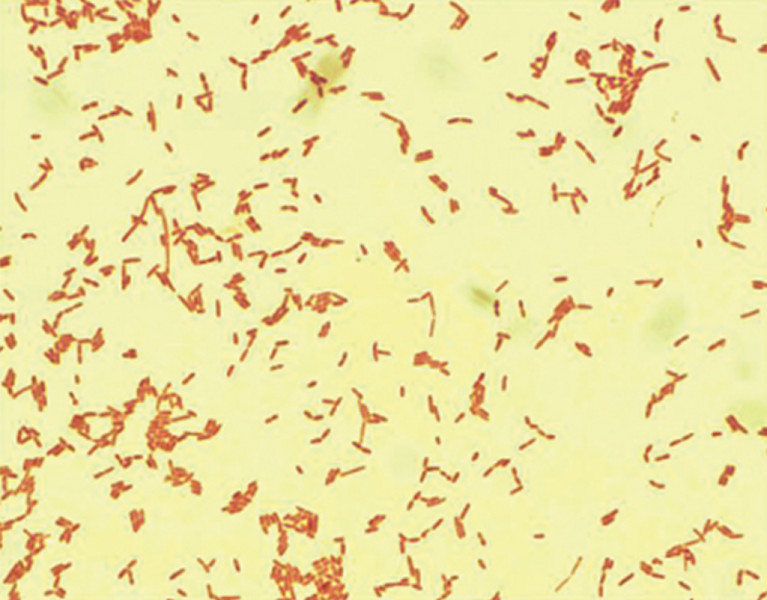
An example of the skin lesions is shown. These are painless puritic papules that have developed into pustules. Edema surronds the pustule and an eschar has developed. A gram stained smear of material from the pustule is shown. The organisms are spore-forming, Gram-positive rods.
m11-2. In a somewhat related case, when Pharaoh did not heed Moses to the let the captive Hebrews go, a series of plagues fell upon the land of Egypt. In the fifth plague, large domesticated mammals including cattle, horses, and sheep died. This was followed by a plague in which the Egyptians developed cutaneous boils. Some developed a mild nonproductive cough associated with fatigue, myalgia, and low grade fever over 72 hours, followed by a rapid onset of severe dyspnea with diaphoresis and cyanosis. Despite antibiotic therapy with both ciprofloxacin and doxycycline (had they been available), many of those affected would die. Which of the following organisms is most likely to have produced these findings?
Clinical history:A 25-year-old man is involved in an accident in which he is ejected from the vehicle. He sustains a compound fracture of the left humerus and undergoes open reduction with internal fixation of the humeral fracture. Several days later, he has marked swelling of the left arm and crepitus.
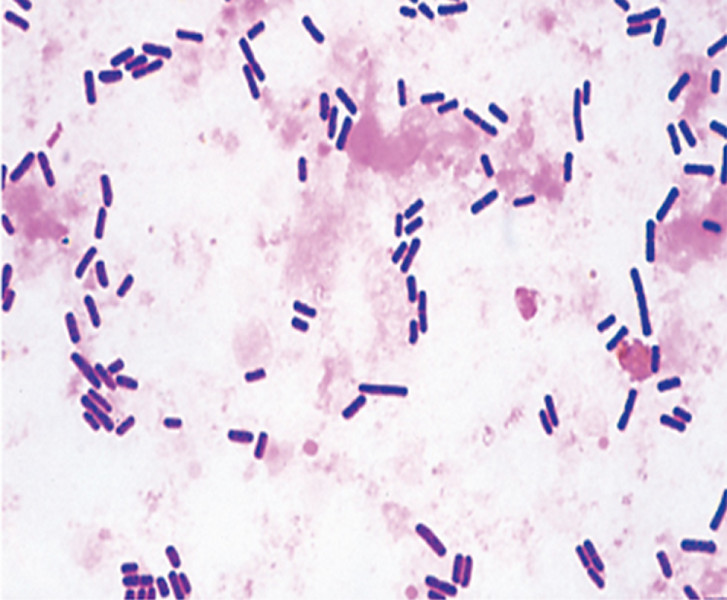
On the arms, there is marked swelling and tissue destruction with black discoloration. Boxcar shaped gram positive rods are seen in the gangrenous tissue. The organism requires anaerobic culture conditions and egg yolk agar for growth.
m13-1. In a similar case, a middle aged woman with type 2 diabetes presents to the emergency room with a very painful right lower leg. She has a wound on that extremity and stated that she stumbled on a fallen tree limb in her yard. You observe that her lower leg is discolored and swollen with several areas of crepitus. The abscess fluid was sent to the microbiology laboratory for aerobic and anaerobic culture. The organism grew best on anaerobic cultures and was lecithinase positive. Gram stain shows gram positive rods and the organism show anaerobic growth on egg yolk agar. What is the most likely organism?
Absolutely critical information you must know to practice medicine is in bold font. Important information that will be needed for routine patient care is in regular font. Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
Discuss the following hereditary disorders, in terms of pathogenesis, morphology, and clinical presentation:
Describe the morphologic sequence of normal bone growth, as well as of repair following fracture of a long bone. Indicate the way(s) in which age, mobility, nutritional state, and infection influence the repair process.
Discuss the following non‑neoplastic bone disorders, in terms of etiology, pathogenesis, morphology, and clinical findings and course:
Absolutely critical information you must know to practice medicine is in bold font. Important information that will be needed for routine patient care is in regular font. Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
Compare and contrast the clinical and pathologic features of :