Website Cases:
Additional Case (NOT assigned):
CASE NUMBER 92
[DigitalScope]
--Click here for a video debrief of the pathology findings presented in this case--
Clinical History: A 65-year-old man presented to the emergency department with sudden onset dyspnea. He reported that he had been experiencing shortness of breath over the last ten years and that he had smoked 2 packs of cigarettes/day since he was 17. His medical history was significant for asthma as a child. He was admitted to the hospital for observation for worsening cardiac function, but experienced a myocardial infarction on the second day and died. Gross and microscopic images from the autopsy are provided.
Image Gallery:
Summary of Gross Findings
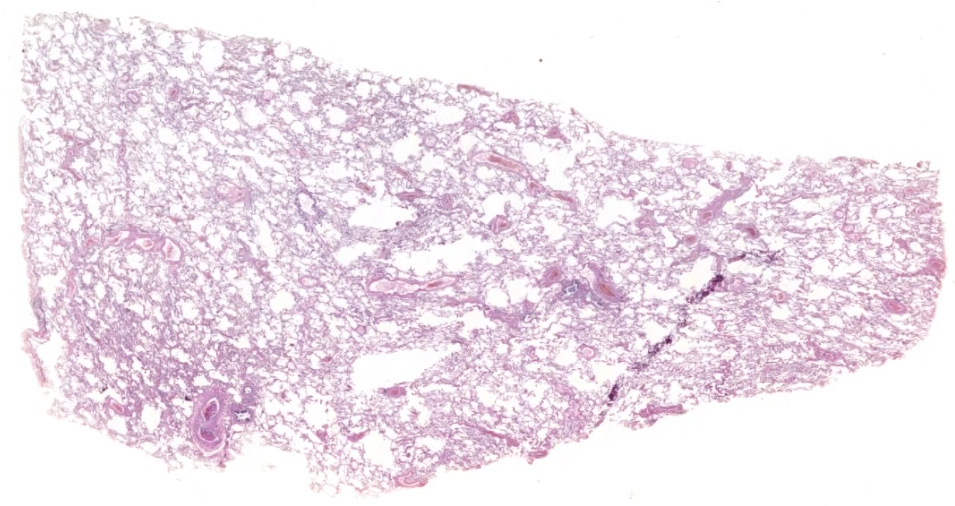
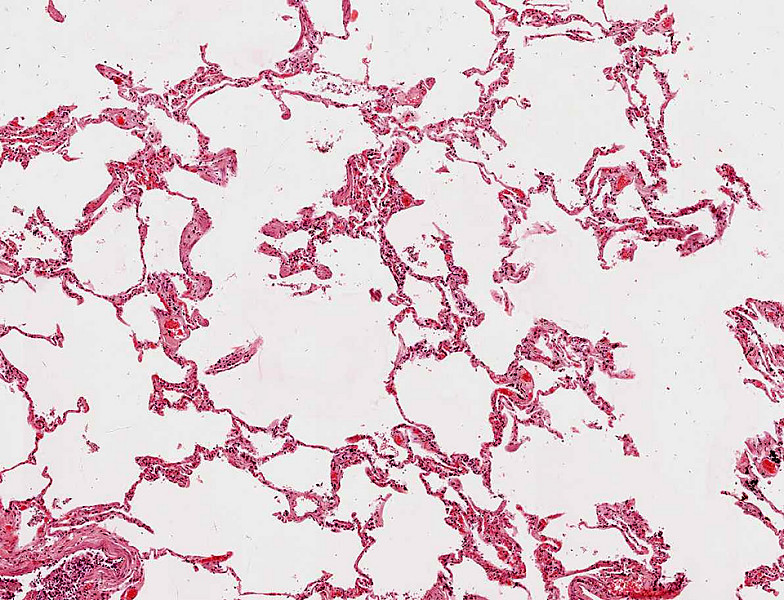
The lungs were very large and upon palpation there was marked crepitation (crackling sound). There is diffuse anthracosis and large, empty spaces showing loss of normal alveolar architecture.
|
Summary of Microscopic Findings
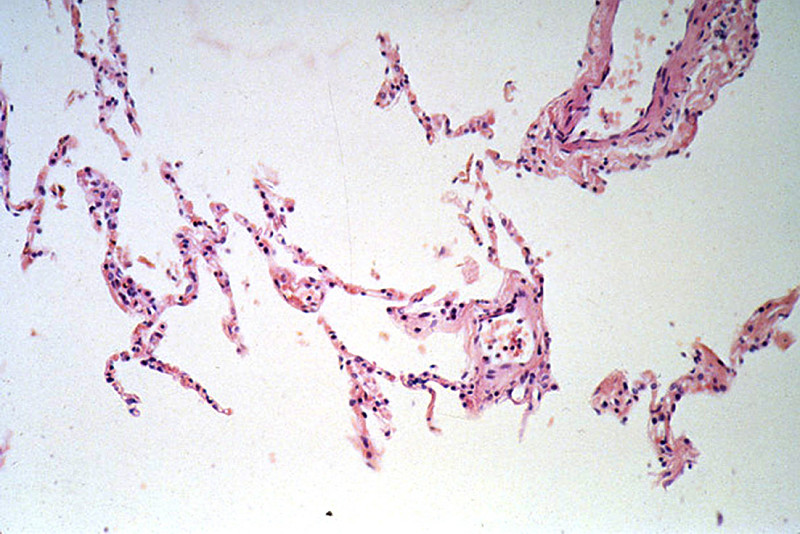
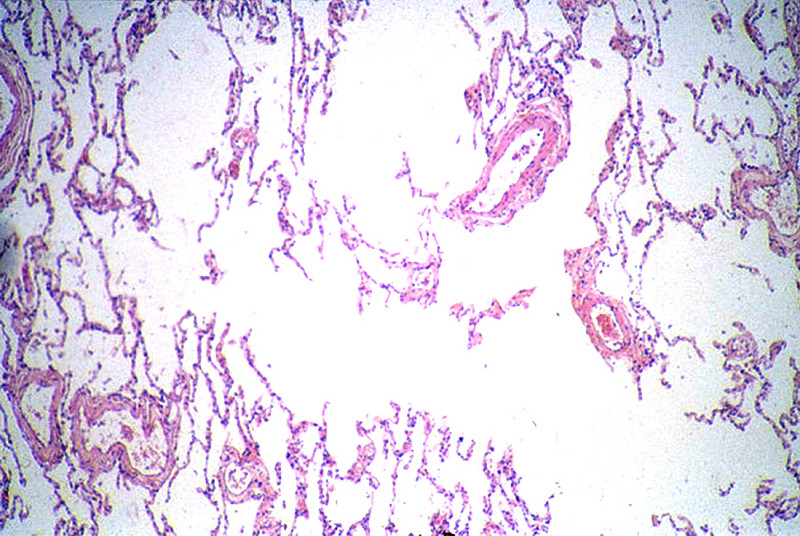
The alveolar spaces are distended and the alveolar septa are thickened by fibrous tissue. Numerous "free floating" alveolar septa are present, recognizable as pieces at alveolar wall not connected at either end to adjacent septa.
|
Review Lung Histology
Norm No. 24 Lung
[ImageScope] [WebScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
|
|
Gross image questions:
- Using a screenshot, annotate the areas of grossly normal and abnormal lung.
- Make a small list, not exhaustive, of what the differential might be.
VM image questions:
- Screenshot and annotate areas of the lung which correlate with the abnormal areas you labeled grossly.
- What is the process occurring in the lung?
- Bonus… look at the small airways and adjacent alveolated tissue. What do you notice that correlates with the patient’s clinical history?
92-1. What is the differential diagnosis?
--ANSWER--
92-2. Which of the following is the most significant risk factor for this patient in the development of his disease?
- α1-antitrypsin deficiency
- Bronchial obstruction
- Cigarette smoking
- History of asthma
- Mutation in the PKD1 gene
--ANSWER--
92-3. Which of the following is considered the most likely mechanism by which lung tissue is damaged in this disease?
- Direct toxicity of tobacco smoke
- Free radical release generated by fibers
- IL-1 and TNF elaboration by macrophages
- Protease release by neutrophils
- Type III hypersensitivity
--ANSWER--
CASE NUMBER 81
[DigitalScope]
--Click here for a video debrief of the pathology findings presented in this case--
Clinical History: A 62-year-old man with an alcohol use disorder presented to his primary care physician with a 3-month history of increased abdominal girth. Physical exam revealed telangiectasias and fluid wave of the abdomen. Laboratory findings showed elevated aminotransferase and decreased serum albumin; no other significant findings were noted. He was admitted to the hospital for further evaluation, but began retching violently with extensive hematemesis. Volume resuscitation failed and the patient died.
Image Gallery:
Summary of Gross Findings
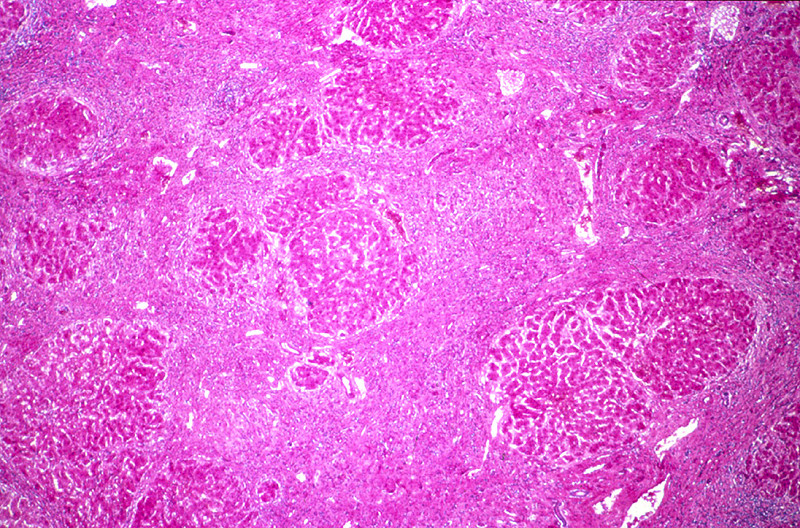
The liver weighed 1800 grams. The entire organ was uniformly composed of nodules about 0.5 cm in diameter, each surrounded by fibrous tissue. The organ was jaundiced and firm.
|
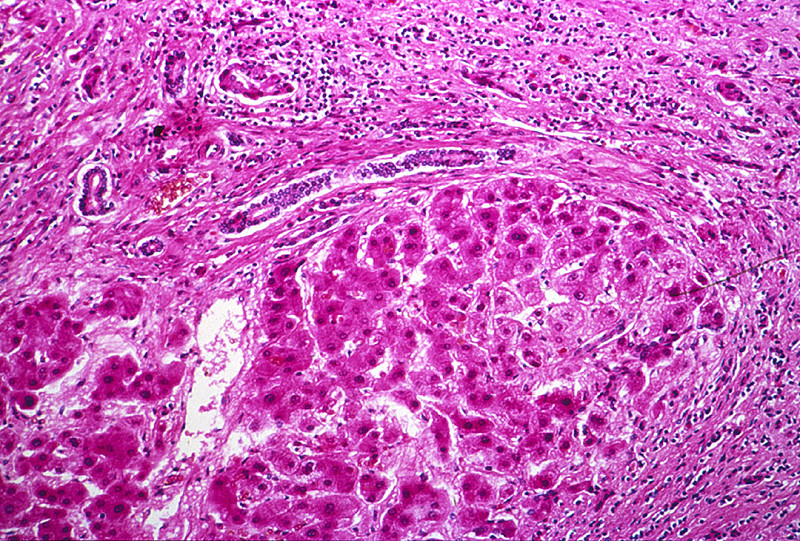
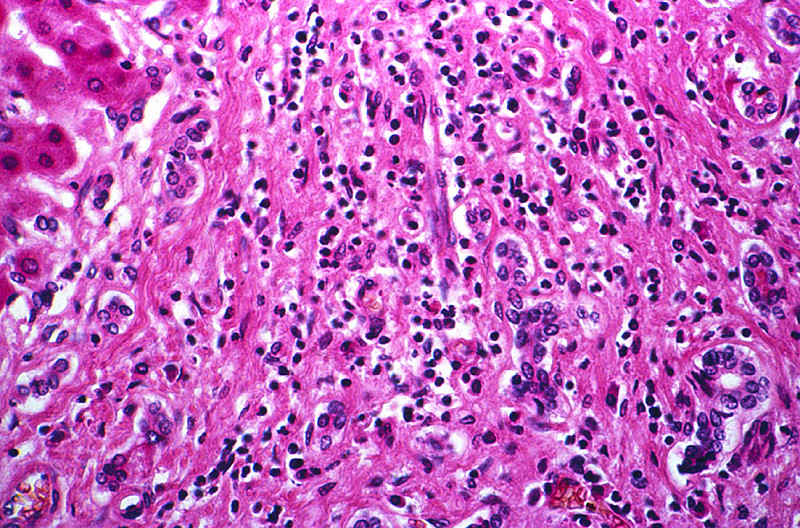
Summary of Microscopic Findings
The usual architecture present in the liver has been completely disrupted by the bands of connective tissue. In these bands one sees chronic inflammatory cells, mainly lymphocytes and other mononuclear cells. There is some proliferation of the bile ductules.
|
Review Liver Histology
Norm No. 3 Liver
[ImageScope] [WebScope]
The liver is the organ that metabolizes nutrients received from the digestive tract. These nutrients and processed by tissue hepatocytes which are large polygonal cells. The hepatocyes are separated by portal triads. The triads consist of an artery, a vein and a bile duct. The bile duct is lined by cuboidal epithelium. The artery has a muscular wall and a flat endothelial lining. The sinuses are well defined and contain a small amount of blood.
|
|
Gross image questions:
- Describe the gross appearance of the liver. Is the process diffuse or localized?
VM image questions:
81-1. What is the differential diagnosis?
--ANSWER--
81-2. Which of the following is the main enzyme involved in alcohol metabolism?
- Acetaldehyde dehydrogenase
- Alcohol dehydrogenase
- Catalase
- Cytochrome P450
- Glutathione peroxidase
--ANSWER--
81-3. Moderate intake of alcohol is most closely associated with which of the following?
- Bitot spots
- Hepatic adenoma
- Leptin secretion
- Nasal ulcers
- Steatosis
--ANSWER--
81-4. Which of the following is the mechanism that leads to the finding in question 3?
- Catalase levels are insufficient for cellular needs
- Decreased NAD+ levels impair fatty acid oxidation
- Endotoxin release stimulates TNF secretion
- Metabolism of ethanol produces reactive oxygen species
- Mucosal epithelium shifts to a squamous morphology
--ANSWER--
CASE NUMBER 98
[DigitalScope]
--Click here for a video debrief of the pathology findings presented in this case--
Clinical History: A 70-year-old man presented to the emergency department with sudden worsening of his dyspnea. He reported that over the last 6 months he had been experiencing dyspnea, orthopnea, paroxysmal nocturnal dyspnea and ankle edema. Further questioning revealed that he worked in a rock quarry as a crusher for 18 years. He was admitted to the hospital for congestive heart failure, but died suddenly of a massive acute myocardial infarction.
Image Gallery:
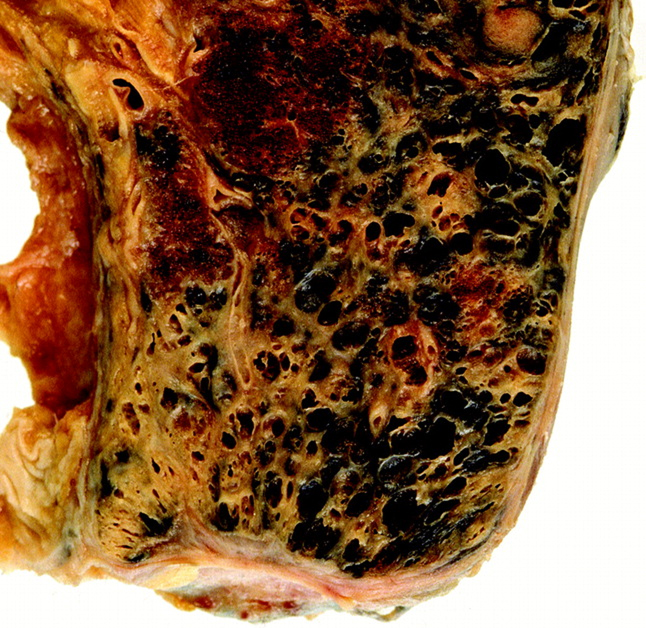
Summary of Gross Findings
Both lungs were heavy, 888 grams for the left lung and 1033 grams for the right one. The cut surface of both lungs shows marked airway centered scarring with variably sized anthracotic nodules involving the upper and lower lobes. Additionally, areas of broad scarring/conglomerate fibrosis are present which measure up to 8 cm in the right lung and 5.5 cm in the left lung.
|
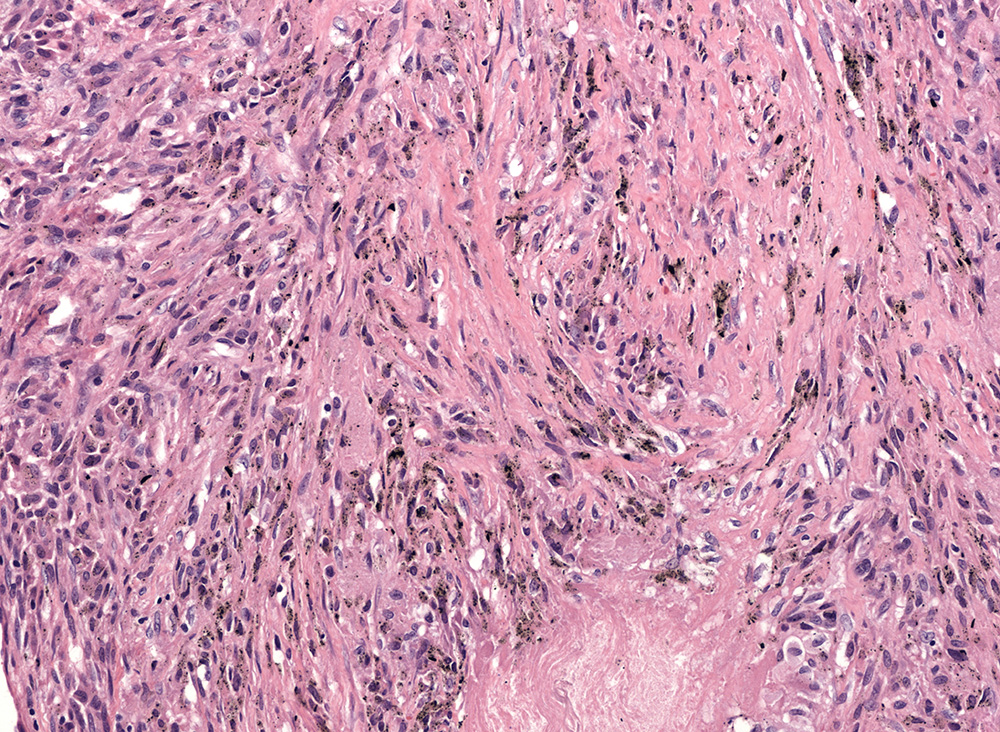
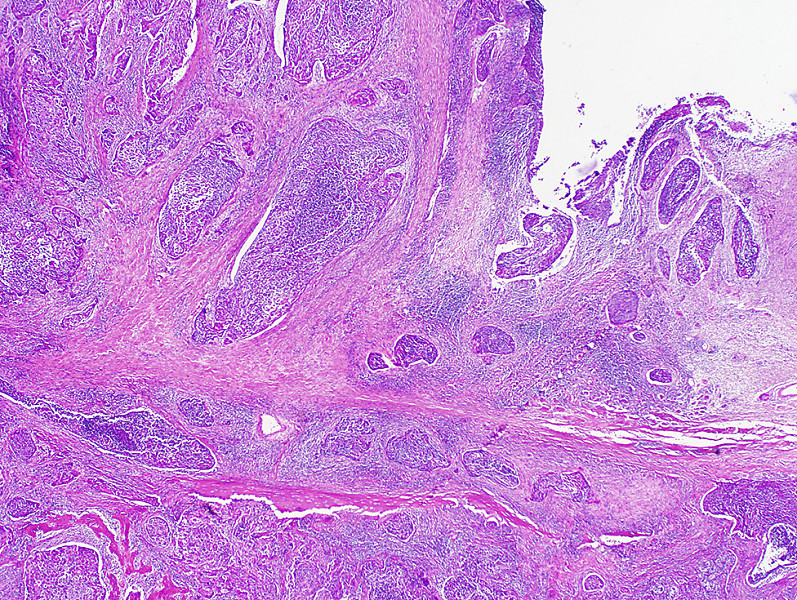
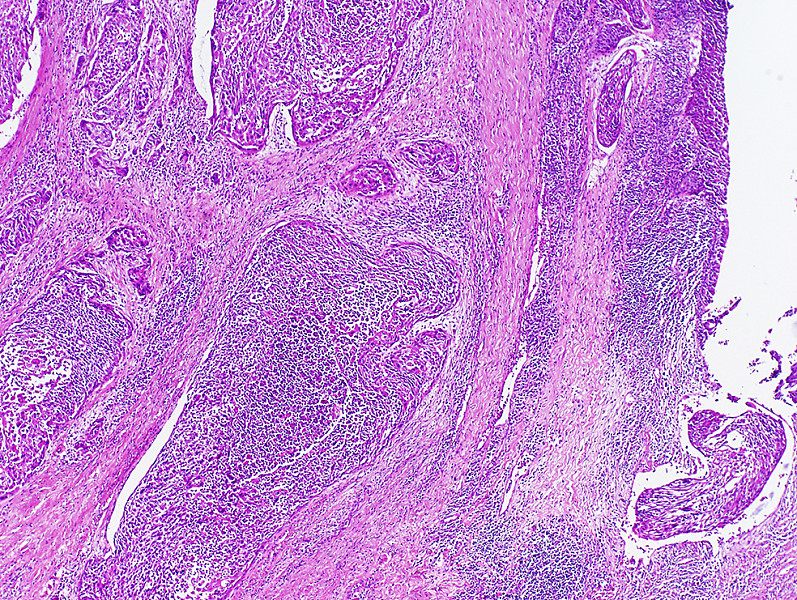
Summary of Microscopic Findings
Review of the virtual microscopy section shows a nice pattern of peribronchovascular and parenchymal dust macules and nodules. One can appreciate and medium and higher magnification carbon dust pigment (black colored material) present within these areas, often accompanied by stellate fibrotic scarring. The still image show dust macules and nodule with central fibrosis, with features characteristic of coal dust macules and nodules. Within these stellate scars, if one were to polarize the tissue, dust particles characteristic of silica and silicates would be seen in abundance. In advanced lesions the fibrous nodules become confluent as seen in the upper lung zone in the gross image.
|
Review Lung Histology
Norm No. 24 Lung
[ImageScope] [WebScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
|
|
Gross image questions:
- Describe the lung characteristics, focusing on the color and pigment.
VM image questions:
- Screen shot and annotate at low power areas of relatively abnormal lung.
- Describe the distribution of disease and the differential for the findings.
- Using the still images, what do these images best represent?
98-1. What is the differential diagnosis?
--ANSWER--
98-2. Which of the following sites is most frequently affected by this disease?
- Bronchial mucosa
- Lower lobes of lungs
- Pleura
- Pulmonary arteries
- Upper lobes of lungs
--ANSWER--
98-3. Which of the following is the most common etiologic agent in this disease?
- Asbestos
- Carbon
- Cigarette smoke
- Micropolyspora faeni
- Quartz
--ANSWER--
98-4. Which of the following cells is most strongly implicated in the development of this disease?
- Endothelial cells
- Macrophages
- Plasma cells
- Smooth muscle cells
- T lymphocytes
--ANSWER--
CASE NUMBER 560
[DigitalScope]
--Click here for a video debrief of the pathology findings presented in this case--
Clinical History: A 72-year-old man was found dead in his home by his wife. She told the medical examiner that he was a retired shipyard worker who had smoked 1 pack of cigarettes/day since he was 19. Autopsy revealed that the cause of death was myocardial infarction.
Image Gallery (slide specimen and images courtesy of the University of Michigan):
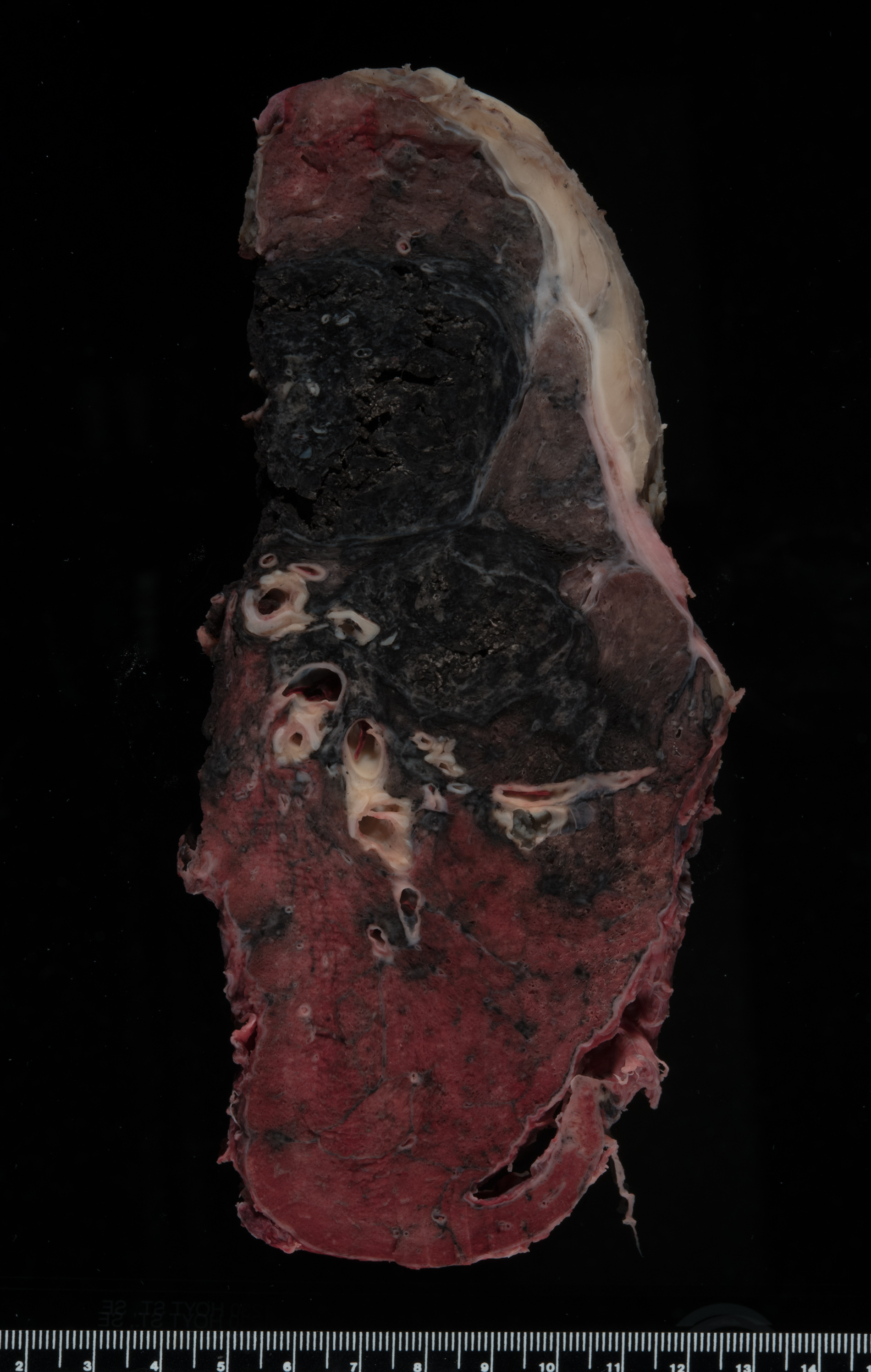
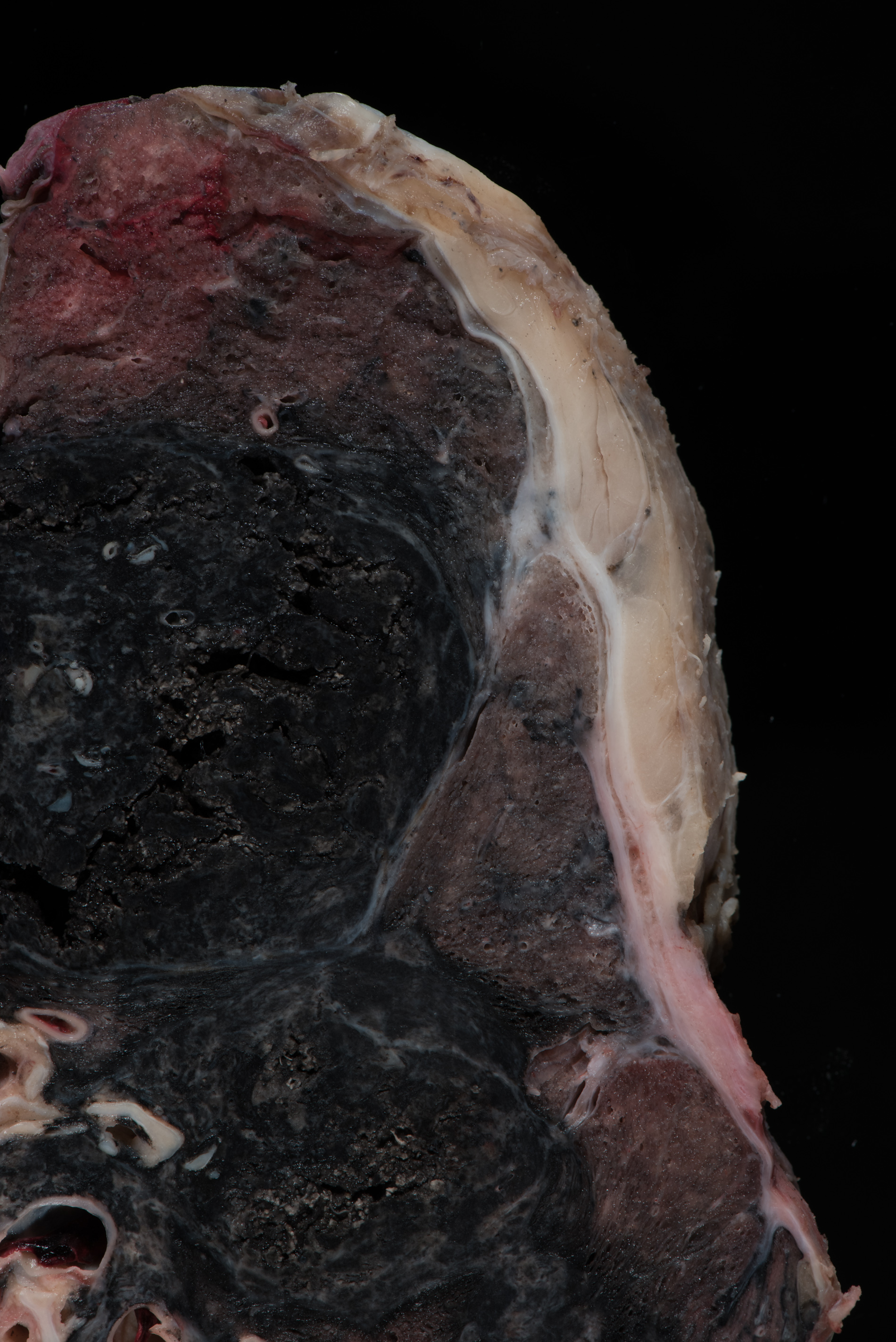
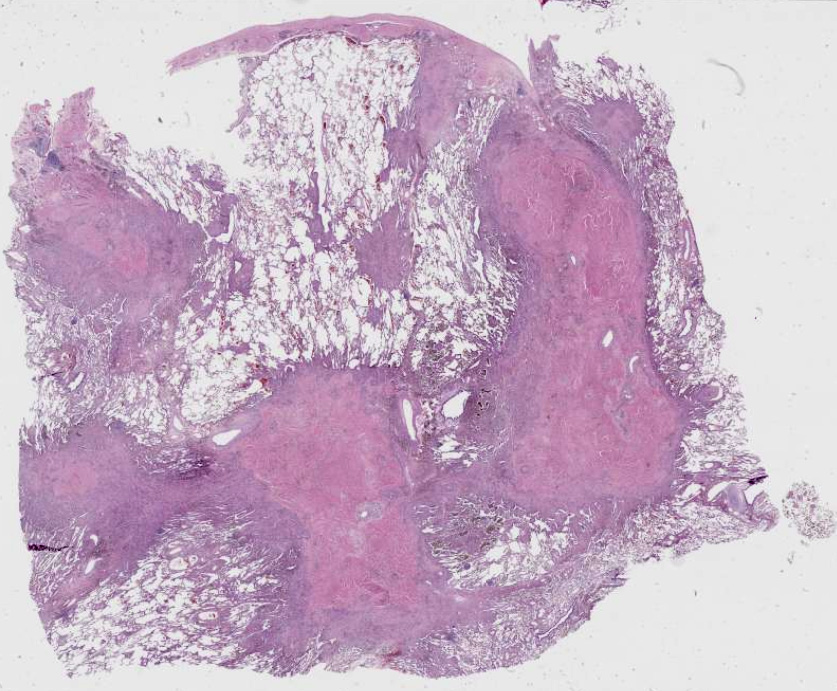
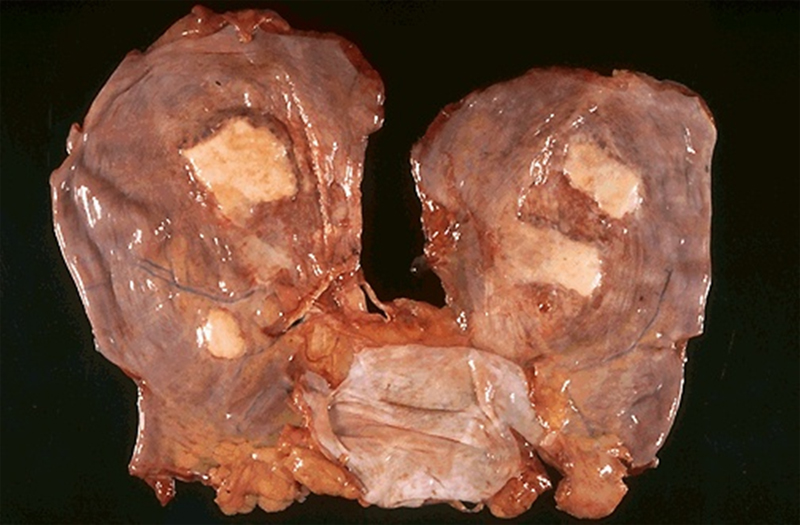
Summary of Gross Findings
This is a section of the diaphragm showing the pleural side. There are dense white fibrocalcific plaques. On cut section, the surface of the lung displays extensive anthracosis with emphysema, and a pattern of coarse parenchymal fibrosis. While somewhat difficult to assess, the fibrotic changes show evidence of a peribronchovascular distribution and extend toward the surface. In the lower left, some more broad areas of scarring is observed, which extends toward central airway structures. The findings raise the possibility of fibrosing parenchymal process.
|
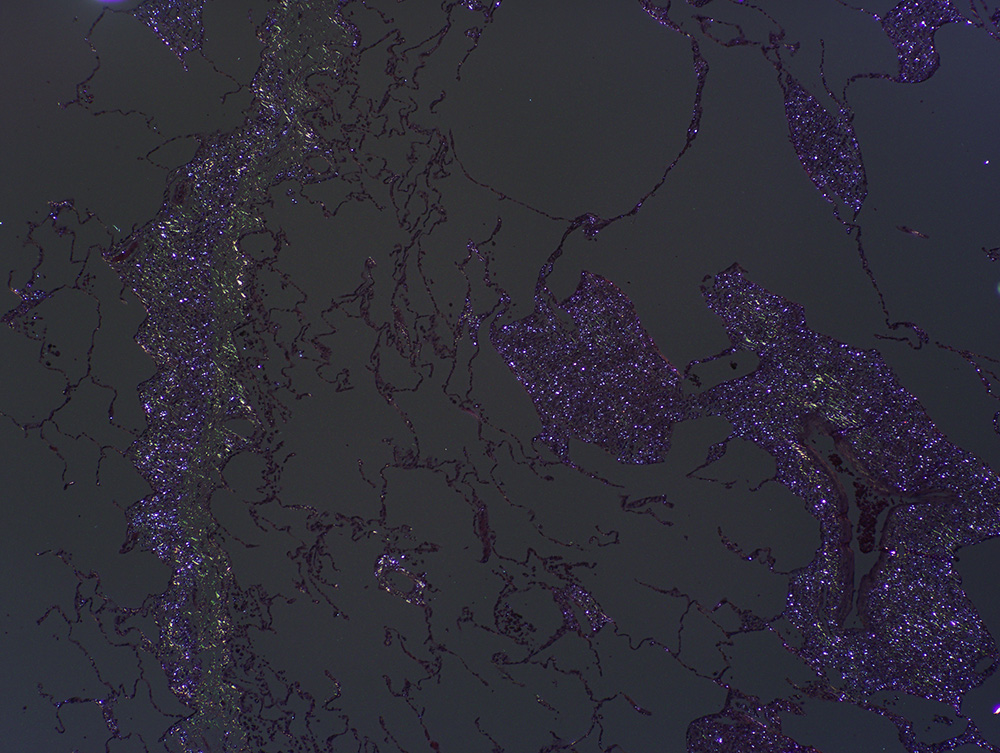
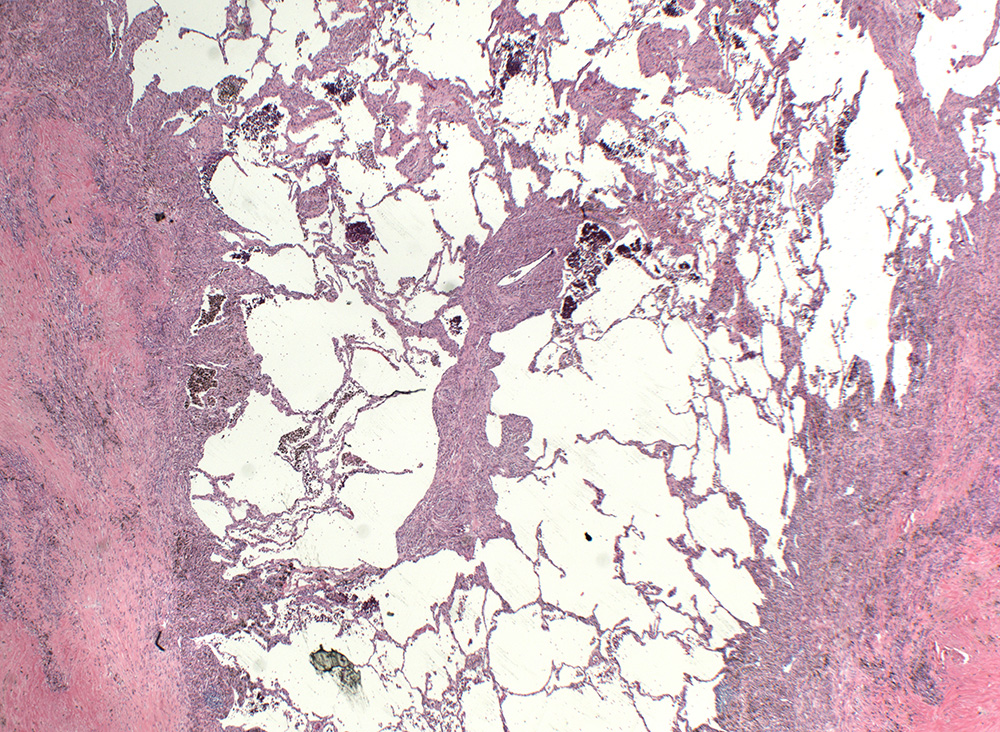
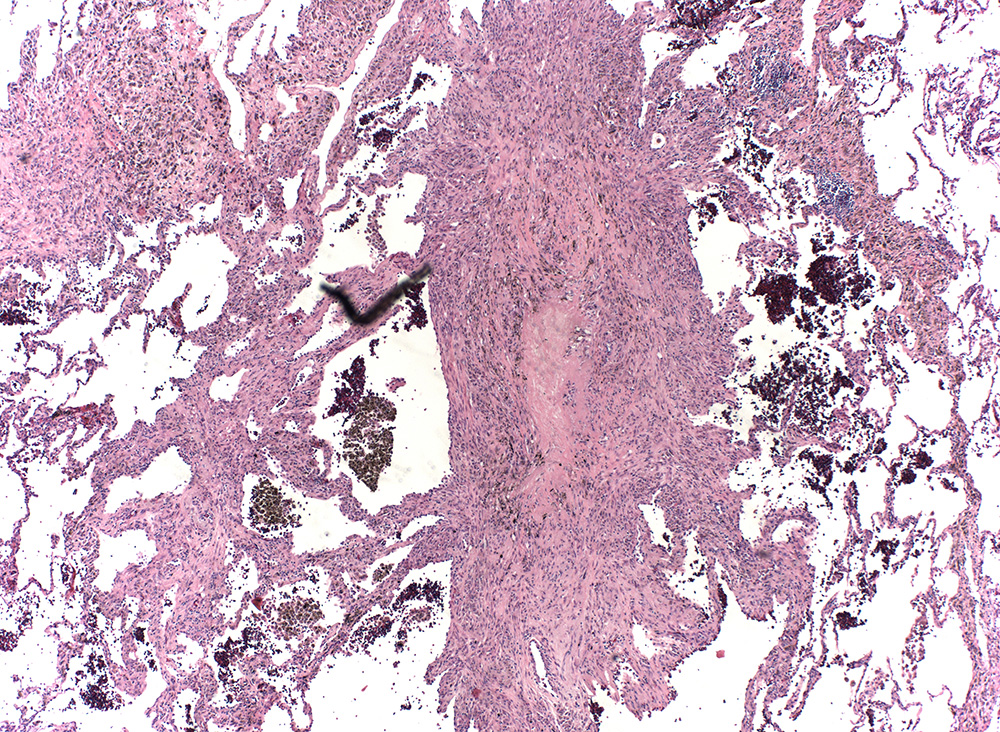
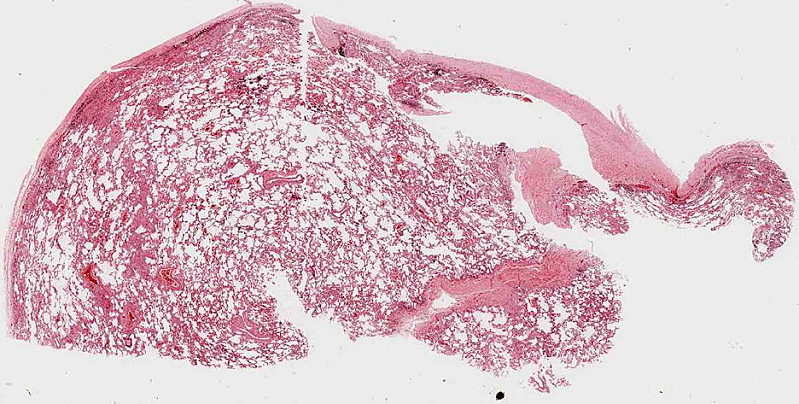
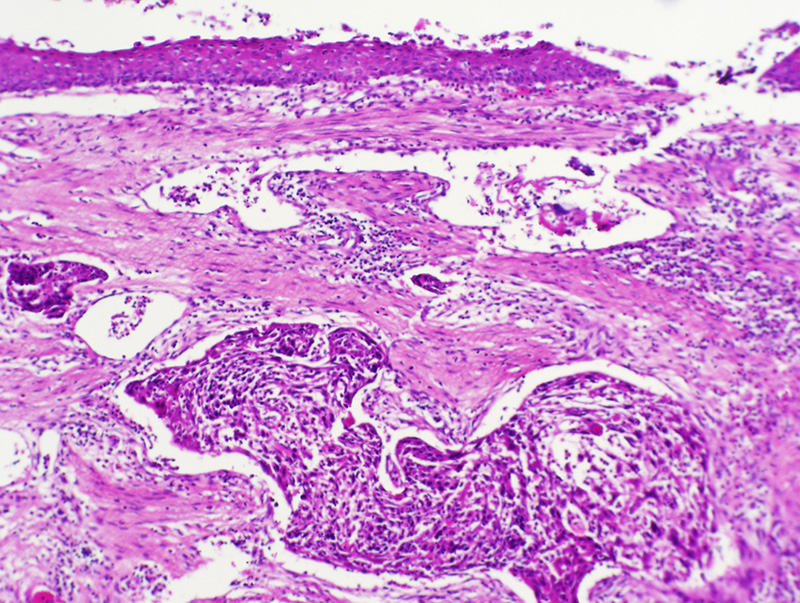
Summary of Microscopic Findings
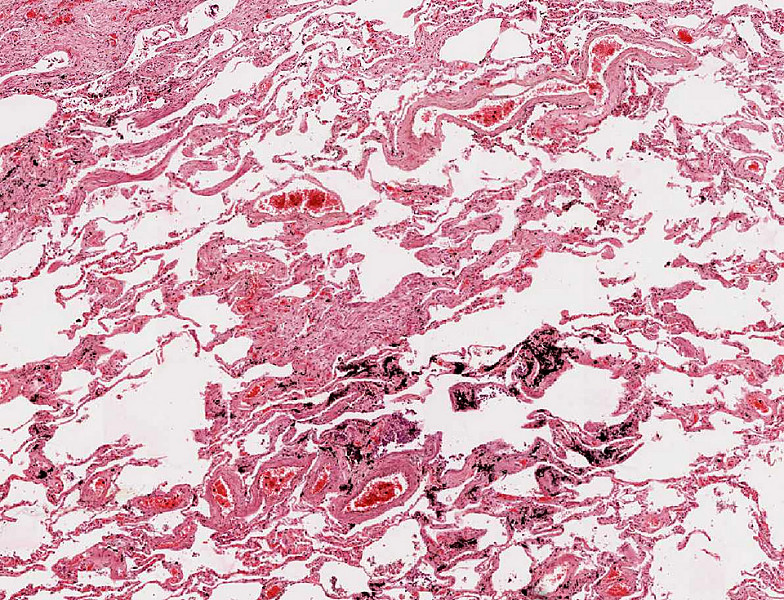
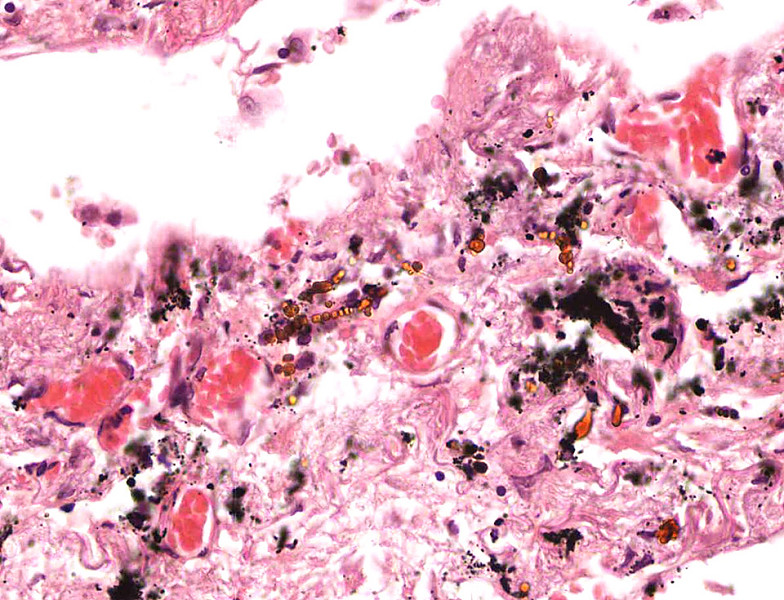
Many of the alveolar walls contain more nuclei than usual and there are detached fragments of alveolar septa. Small deposits of anthracotic pigment are also evident. Many of the alveolar septa are thickened by fibrosis. Within these areas of fibrosis are golden brown beaded or 'knobby' structures.
|
Review Lung Histology
Norm No. 24 Lung
[ImageScope] [WebScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
|
|
--Click here for a video debrief of the pathology findings presented in this case-- Gross image questions:
- What structure is the first gross image depicting?
- Screen shot and annotate areas of normal and abnormal tissue. What process may be going on here that correlates with the patient’s occupational history?
- In the 2nd photo, briefly describe the changes you see in the lung.
- What might be in your differential regarding the patient’s parenchymal lung disease? Why?
VM image questions:
- Screen shot and annotate:
- 1) normal areas of lung and pleura
- 2) abnormal lung and pleura, and
- 3) higher power view of anthracosis and an asbestos body.
560-1. What is the differential diagnosis?
--ANSWER--
560-2. What are the golden-brown objects seen in the microscopic images?
- Beryllium fragments
- Charcot-Leyden crystals
- Ferruginous bodies
- Fungal spores
- Hyaline membranes
--ANSWER--
560-3. Patients with this disease are at greatest risk for developing which of the following complications?
- Acute interstitial pneumonia
- Bronchogenic carcinoma
- Diffuse alveolar damage
- Hypersensitivity pneumonitis
- Sarcoidosis
--ANSWER--
560-4. Which of the following pulmonary function test results is consistent with this patient’s diagnosis?
- Decreased forced vital capacity
- Decreased maximal expiratory flow rate
- Increased forced expiratory volume at 1 second
- Increased residual volume
- Increased total lung capacity
--ANSWER--
CASE NUMBER 154
[DigitalScope]
Clinical History: A 64-year-old man presented to his primary care physician with a two-month history of increasing hoarseness. Additional findings elicited in his history and physical include:
- 50-pack year smoking history
- hepatitis B infection; and
- work in a shipyard
Upper endoscopy revealed an ulcerated mass at the level of the vocal cords. A laryngectomy was performed.
Image Gallery:
Summary of Gross Findings
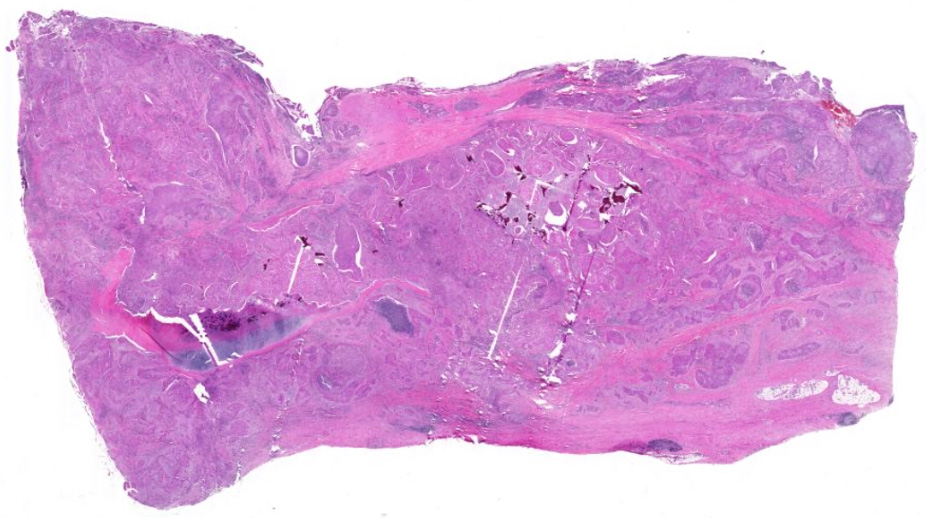
An ulcerated tumor involved the left true and false vocal cords and extended across the midline.
|
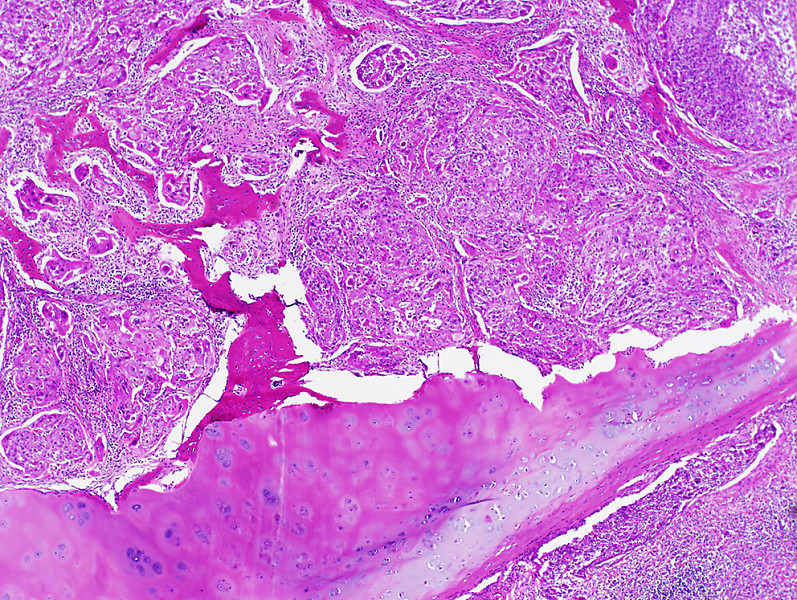
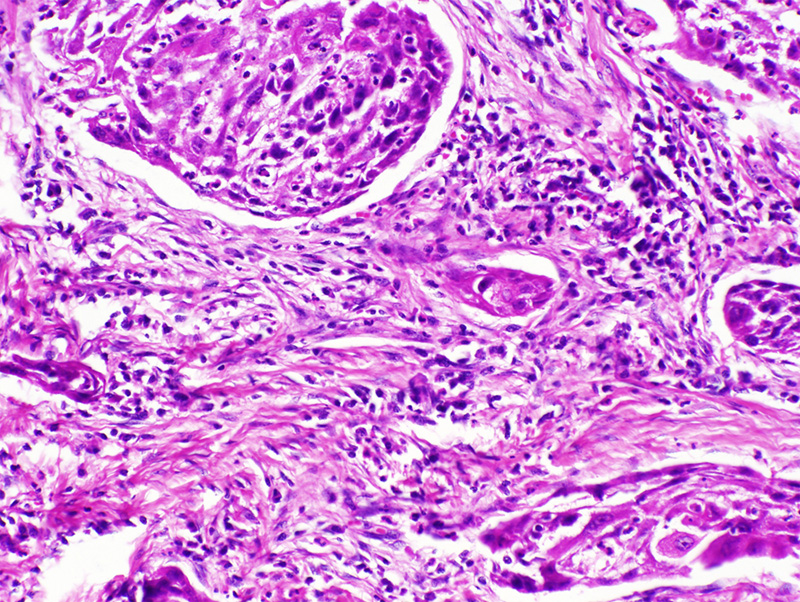
Summary of Microscopic Findings
The mucosa is partially columnar, representing the ventricular mucosa. There is a transition to squamous mucosa with marked nuclear pleomorphism. The abnormal squamous cells extend into the underlying stroma where the cells keratinize. Focal necrosis and an inflammatory infiltrate are present.
|
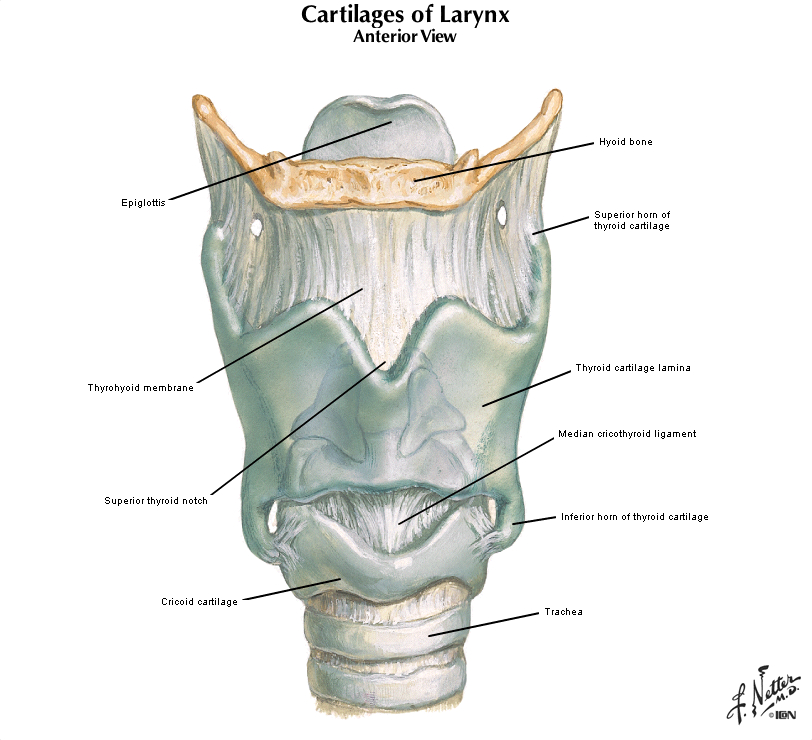
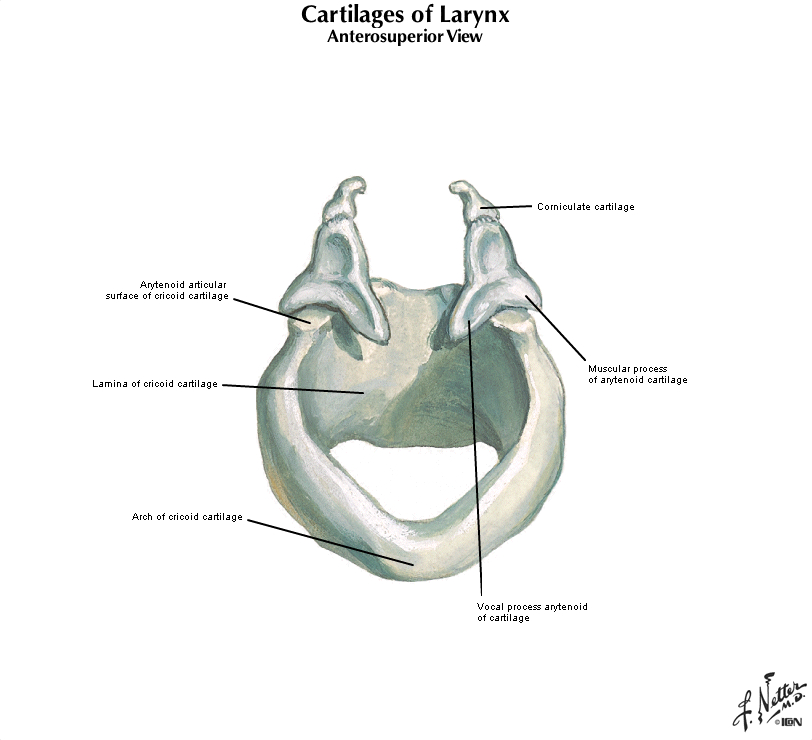
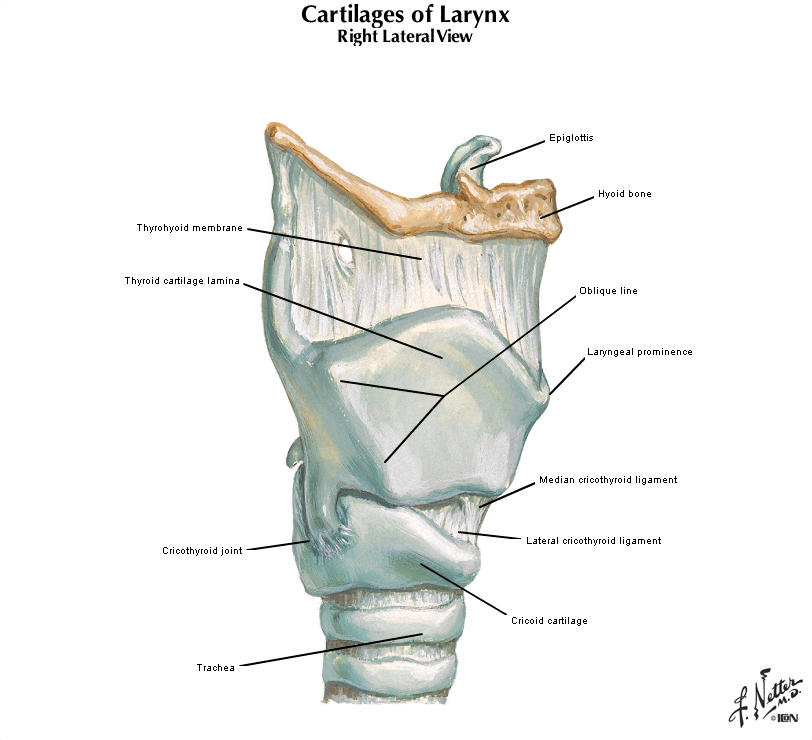
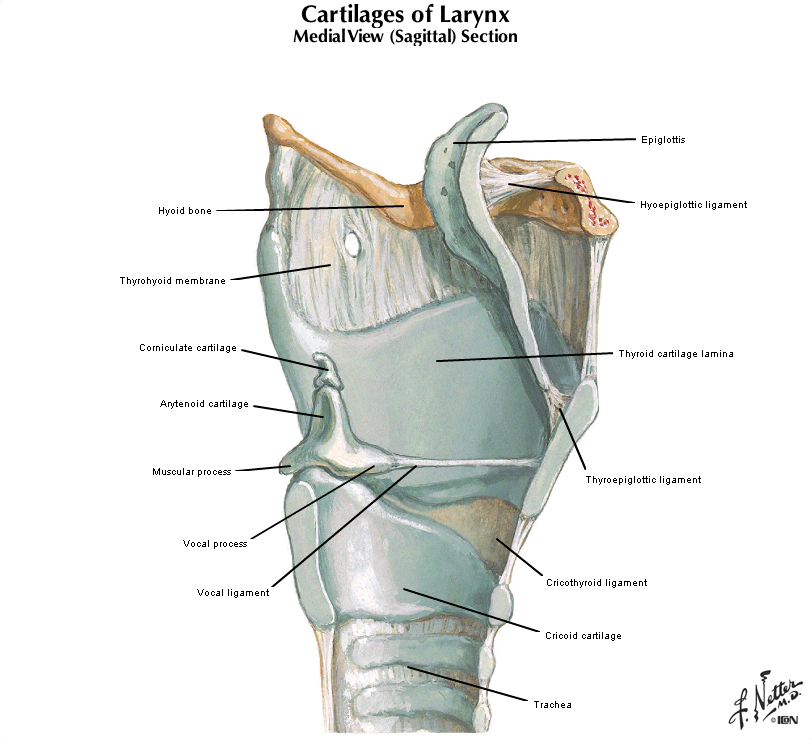
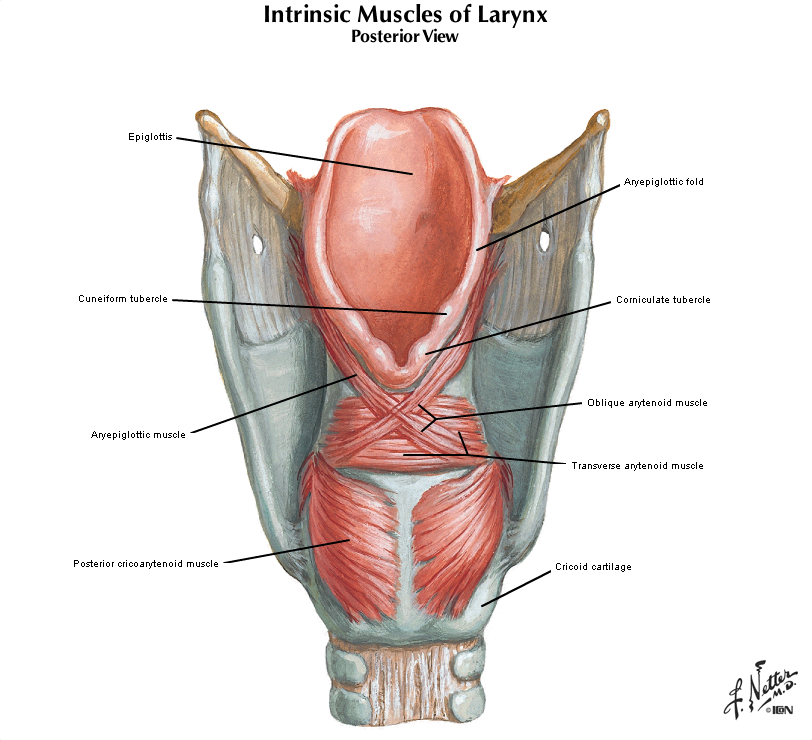
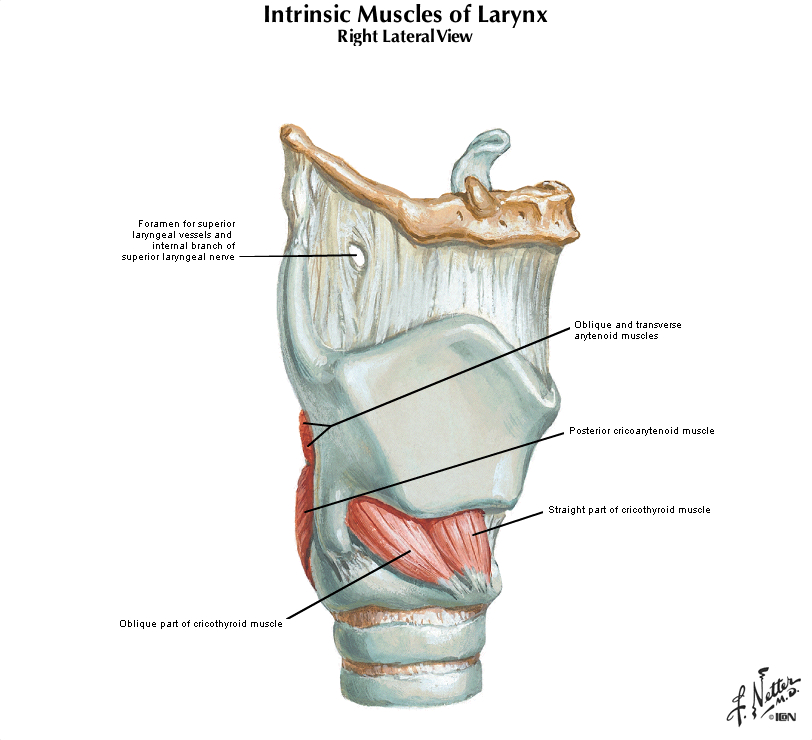
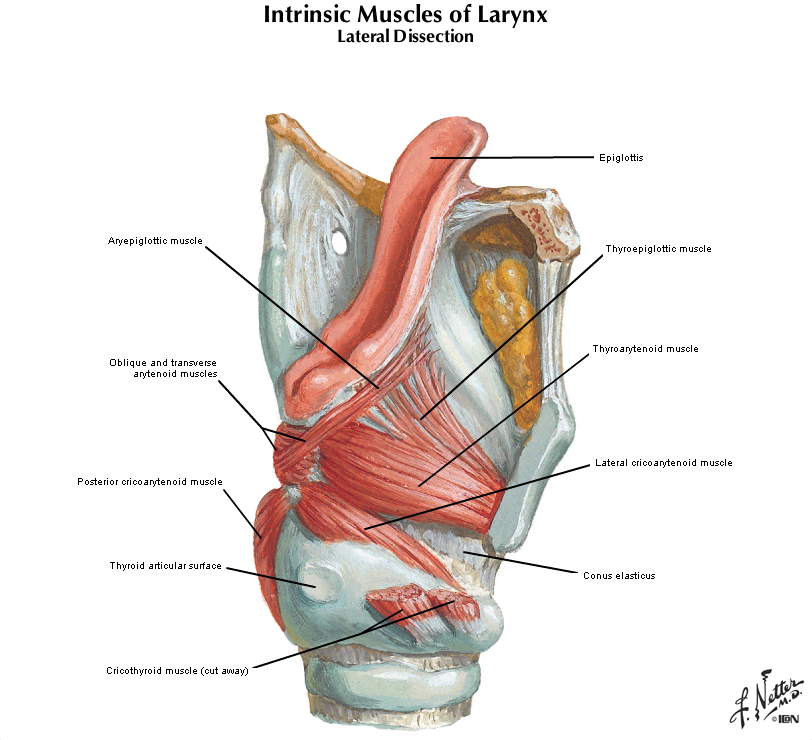
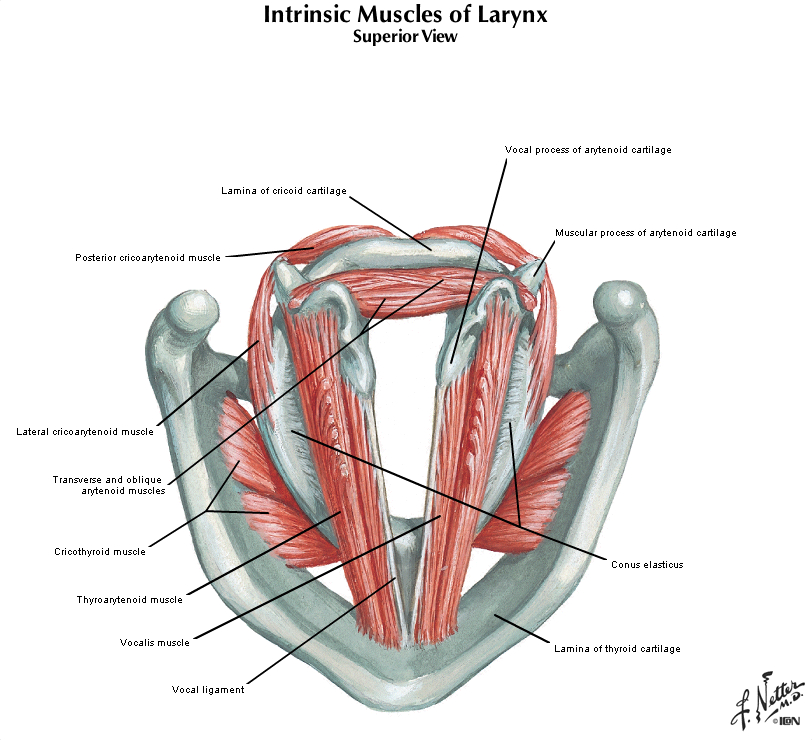
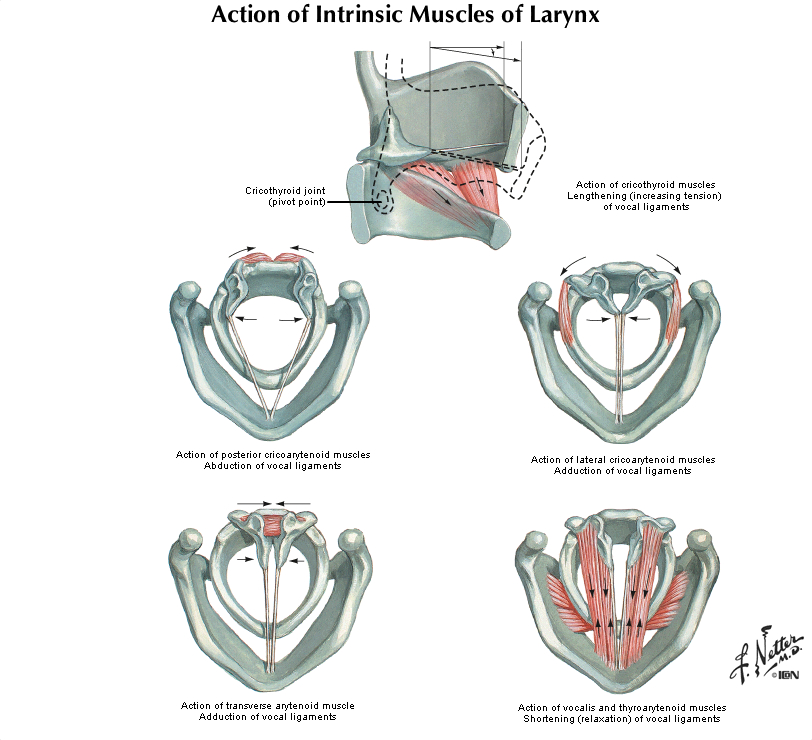
Review Larynx Histology
Slide 307 - Larynx
[ImageScope] [WebScope]
The larynx is a passageway for air between the oropharynx and trachea which also functions in the production of sound. It is lined by pseudostratified columnar epithelium (see left hand side of the slide), stratified squamous epithelium (covering the vocal cords near the middle of the slide), and stratified columnar epithelium between these epithelial types. Seromucous glands are present underneath the epithelium on both sides of the slide. Identify the vocal cord as a mucoal fold covered by stratified squamous epithelium and containing abundant skeletal muscle. Superior to the vocal fold (to the right of the focal fold on this slide) is the vestibular fold (aka "false" vocal fold), which is lined by respiratory epithelium. Notice the cartilage framework, within which there is some ossification as occurs as part of the aging process (this specimen is from a 62-year-old).
|
|
Gross image questions:
- On the gross specimen, identify the epiglottis, the hyoid bone, and the mass.
--Click here for a video debrief of the pathology findings presented in this case--
154-1. What is the differential diagnosis?
--ANSWER--
154-2. Which of the following risk factors is MOST closely linked to this disease?
- Asbestos exposure
- Gastroesophageal reflux disease
- Hepatitis B infection
- Tobacco smoking
- Vitamin C deficiency
--ANSWER--
154-3. Recent studies have correlated HPV infection with oropharyngeal squamous cell carcinoma. Which of the following accounts for the carcinogenesis of high-risk HPV infection?
- Loss of function mutations in cyclin-dependent kinase inhibitors
- Dysregulation of MYC
- Displacement of E2F transcription factors from RB
- Gain of function of CDK4
- Stabilization of p53
--ANSWER--
ENVIRONMENTAL PATHOLOGY Review Items
Key Vocabulary Terms (click here to search any additional terms on Stedman's Online Medical Dictionary)
LEARNING OBJECTIVES
Goal 1: Cell Injury
Apply knowledge of biochemistry, and cellular physiology to describe the mechanisms leading to cell injury induced by exposure to external agents including radiation, environmental toxins, drugs of abuse, and therapeutic agents.
- Objective 1: Mechanisms of Cell Injury
Compare and contrast different mechanisms of chemical injury, specifically agents that act by direct binding to and inactivation of cellular constituents with those that require metabolic activation to induce toxicity and discuss how genetic factors affect toxicity of different agents.
- Objective 2: Tobacco Use
Discuss the pathogenesis of tobacco use and the resultant pathologic changes in affected organs.
- Objective 3: Alcohol Use
Discuss the pathogenesis of alcohol abuse and the resultant pathologic changes in affected organs.
- Objective 4: Drugs of Abuse
Describe the mechanism by which drugs of abuse induce central nervous system effects, and discuss, with examples, toxicities associated with both chronic use and acute overdose of these drugs.
- Objective 5: Occupational Exposure
Provide examples of industrial, occupational or environmental exposures that produce disease, and indicate the organ systems are most commonly affected by which agents.
- Objective 6: Toxicity of Therapeutic Drugs
Discuss, with examples, how therapeutic drugs can produce toxic effects on different tissues, distinguishing between idiosyncratic and dose-dependent effects.
- Objective 7: Radiation
Discuss mechanisms by which radiation damages cells and tissues, and compare and contrast how ultraviolet radiation, therapeutic radiation, and acute radiation sickness produce different disease manifestations in different organ systems.
Goal 2: Physical Injury
Apply knowledge of biochemistry, anatomy, physiology, and mechanisms of cell injury to describe the pathogenic mechanisms of physical injury.
- Objective 1: Mechanical Force Injury
Compare and contrast the types of injuries associated with mechanical force with respect to effects on skin, blood vessels and the directly affected organs, and discuss systemic response to massive trauma.
- Objective 2: Thermal Injury
Discuss thermal injuries, comparing and contrasting the direct and systemic effects of thermal burns, hyperthermia, and hypothermia.
|