Website Cases:
CASE NUMBER 1
[DigitalScope]
Clinical History: A 50-year-old woman presented to the emergency department with a one-month history of flank tenderness and vague abdominal pain. Physical exam revealed palpable kidneys and ultrasound showed cystic changes in both kidneys. Urinalysis showed 2+ proteinuria. The patient progressed to end stage renal failure and was maintained on dialysis until a transplant kidney became available. Gross and microscopic images of the explanted kidney are provided.
Image Gallery:
Summary of Gross Findings
This is a complete hemi section of a markedly enlarged kidney. Examination reveals that the entire kidney is replaced by multiple cysts up to several centimeters in diameter. The cysts are filled with fluid.
|
Summary of Microscopic Findings
This slide is not exactly representative of the impressive gross pathology. Microscopic examination shows variably sized cortical cysts. Typically, these are lined by cuboidal to flattened epithelium (i.e.they are true cysts). There is mild interstitial fibrosis that can become significant in advanced disease. The glomeruli adjacent to the cysts show mild compression.
|
(Review Kidney Histology)
Slide No. 2 kidney
[DigitalScope]
Slide 240 kidney
[DigitalScope]
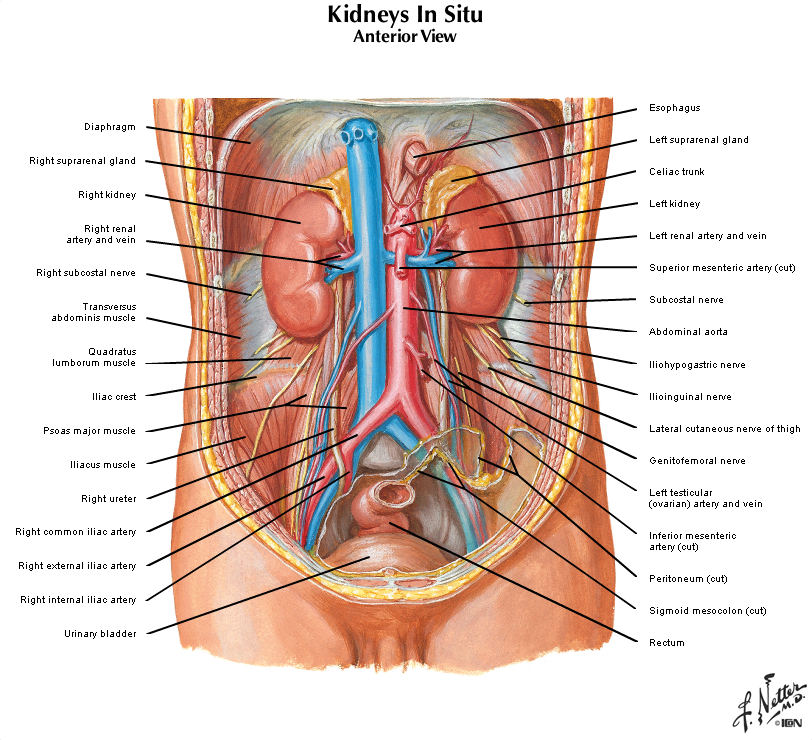
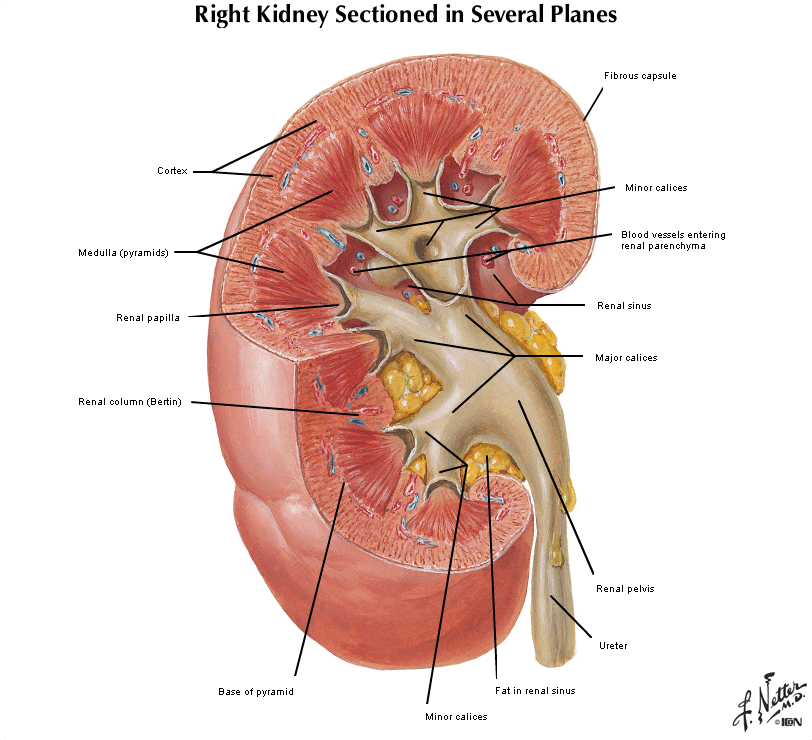
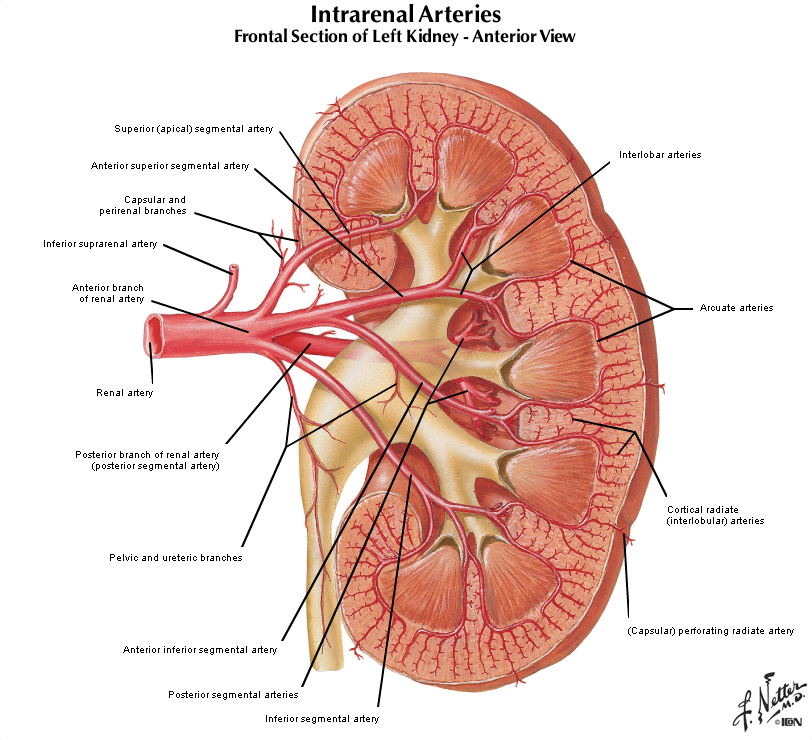
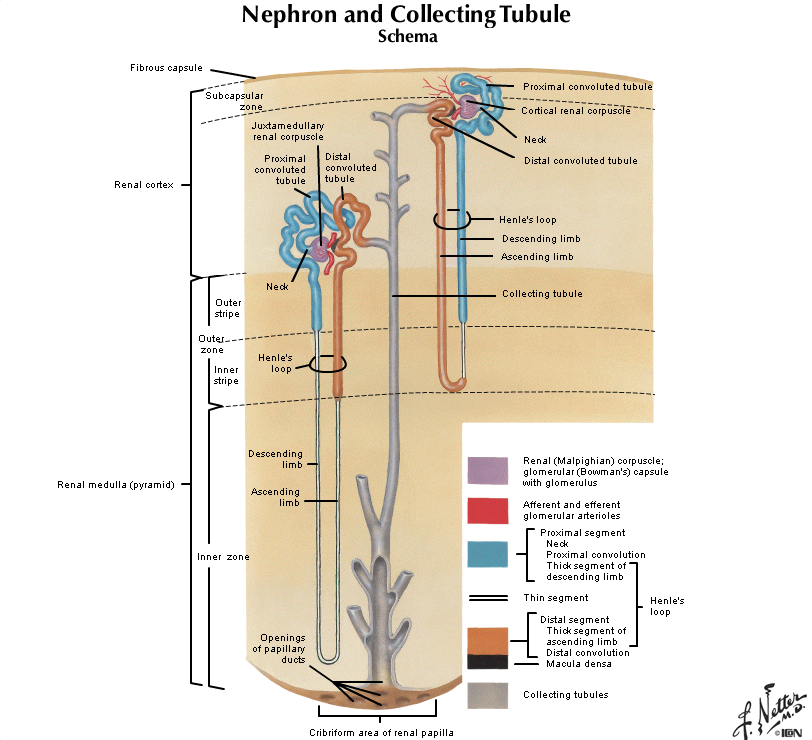
The kidney excretes soluble waste from the body and controls electrolyte balance. It consists of the cortex and the medulla. Within the outer cortex, glomeruli with delicate capillary loops are seen. The basement membrane is thin and without inflammation or thickening. Bowmans capsule that surrounds the glomerulus is thin. The interstitium demonstrates no evidence of inflammation or fibrosis. In the areas between the glomeruli, tubules and arterioles are seen. The tubules are intact. The vessels exhibit no narrowing or wall thickening. The inner medulla of the kidney contains only tubules and blood vessels. Larger arteries and veins are located at the interface between cortex and medulla.
|
|
Gross Questions
- Annotate the gross image indicating the orientation of the kidney (i.e. superior, inferior, etc),
- briefly describe what you observe.
VM Slide Questions
Review the digital scope images of the kidney and annotate:
- a glomerulus, blood vessels, and tubules,
- renal cortex and medulla, and
- areas of cystic change (describe the cyst features)
1-1a. What is the differential diagnosis based on initial presentation?
1-1b. Based on the clinical exam and imaging findings?
1-1c. What is the final diagnosis?
--ANSWER--
1-2. Which of the following genetic abnormalities is most likely to be the etiology this patients disease?
- Autosomal dominant mutation
- Autosomal recessive mutation
- Genomic imprinting
- Germline mosaicism
- Random X inactivation
--ANSWER--
1-3. Which of the following genes is most likely mutated in this patient?
- CFTR
- FBN1
- PAH
- PKD1
- PKHD1
--ANSWER--
1-4. This patient is at greatest risk for which of the following?
- Aortic stenosis
- Hepatic fibrosis
- Hypertension
- Portal hypertension
- Renal cell carcinoma
--ANSWER--
CASE NUMBER 6 - slide courtesy of UIndiana
[DigitalScope]
Clinical History: A 2-year-old girl is brought to the pediatrician by her parents who noticed that she had a large right-sided abdominal mass. A CT scan was performed. Subsequently, the patient underwent a nephrectomy.
Image Gallery:
Summary of Imaging Findings
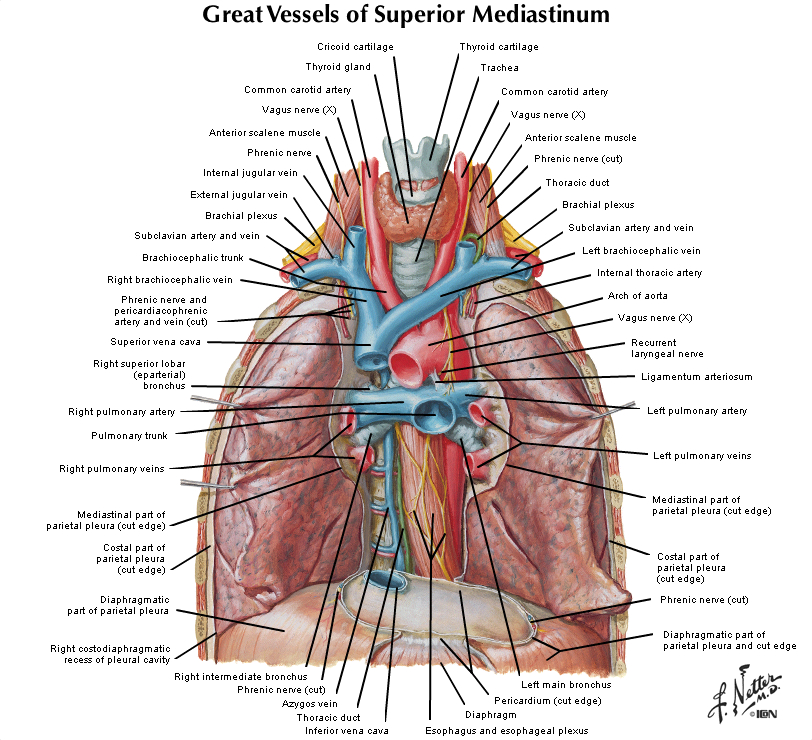
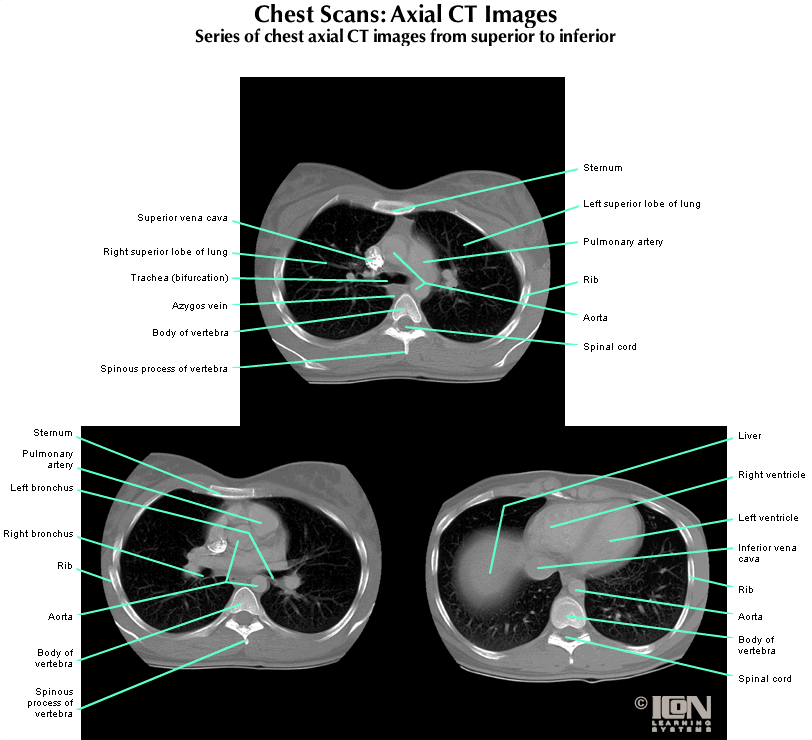
The CT scan shows a heterogeneous mass arising from the right kidney. A small sliver of residual kidney can be seen superomedial to the mass. Note: IV contrast is seen filling the heart and great vessels in the mediastinum and oral contrast was also used to look for possible bowel obstruction (can see oral contrast in large bowel loops inferior to the mass on the right and also just inferior to the spleen on the left).
|
Summary of Gross Findings
Grossly, there is a solitary heterogeneous, lobulated, yellow-tan mass that distorts the kidney. The tumor appears well circumscribed. There are areas of hemorrhage and necrosis. Residual kidney can be seen at the top of the image.
|
Summary of Microscopic Findings
The slide shows a portion of normal kidney. The tumor displays triphasic histology: blastemal (small blue cells), stromal (spindle cells that are fibroblastic and often myxoid which is to say mucoid) and epithelial (glomerular structures and abortive tubules). Heterologous elements such as adipose tissue, cartilage and osteoid, are not seen here.
|
Review Kidney Histology
Slide No. 2 kidney
[DigitalScope]
Slide 240 kidney
[DigitalScope]
The kidney excretes soluble waste from the body and controls electrolyte balance. It consists of the cortex and the medulla. Within the outer cortex, glomeruli with delicate capillary loops are seen. The basement membrane is thin and without inflammation or thickening. Bowmans capsule that surrounds the glomerulus is thin. The interstitium demonstrates no evidence of inflammation or fibrosis. In the areas between the glomeruli, tubules and arterioles are seen. The tubules are intact. The vessels exhibit no narrowing or wall thickening. The inner medulla of the kidney contains only tubules and blood vessels. Larger arteries and veins are located at the interface between cortex and medulla.
|
|
Radiology Questions
- What are the significant findings on the CT scan?
- Identify: the left main stem bronchus, the spleen, the liver, the mass lesion and the residual right kidney (this one is hard).
Gross Questions
- How would you describe the gross specimen? Is it homogeneous or heterogeneous? Does there appear to necrosis? Hemorrhage? Where is the residual kidney?
VM Image Questions
- Describe the microscopic appearance.
- Is there normal kidney?
- How would you describe the lesion?
- Identify the three different cell populations typical of this entity.
6-1a. What is the differential diagnosis based on the patient’s initial presentation?
6-1b. Following the imaging studies?
6-1c. What is the final diagnosis and why?
--ANSWER--
6-2. Which of the following is most closely associated with poor prognosis in patients with this disease?
- Deletion of phenylalanine codon at position 508 (deltaF508)
- Diffuse anaplasia
- Intrauterine exposure to phenylalanine
- NMYC amplification
- X-linked inheritance
--ANSWER--
6-3. Which of the following genes is most commonly mutated in this tumor?
- CFTR
- FMR1
- IGF2
- RB
- WT1
--ANSWER--
6-4. Which of the following entities, associated with this tumor, is a disorder of genomic imprinting?
- Beckwith-Wiedemann syndrome
- Denys-Drash syndrome
- Fragile X syndrome
- Klinefelter syndrome
- WAGR (Wilms tumor, aniridia, genital abnormalities and mental retardation) syndrome
--ANSWER--
CASE NUMBER 539
[DigitalScope]
Clinical History: A newborn baby is noted to have meconium ileus. His mother notices that when she kisses him, his skin tastes salty. A sweat chloride test was 110mEq/L (nl <60 mEq/L). Throughout childhood, he experiences persistent lung infections, chronic cough and obstructive pulmonary disease and, later in life, he develops exocrine pancreatic insufficiency with manifestations of malabsorption. He dies from cor pulmonale and an autopsy is performed.
Image Gallery:
Summary of Gross Findings
The bronchioles are extremely dilated and there are areas with extensive mucus plugging. The pulmonary parenchyma is consolidated by a combination of pneumonia and secretions.
|
Summary of Microscopic Findings
The bronchioles are dilated and filled with mucus admixed with abundant acute and chronic inflammatory cells. There is marked hyperplasia and hypertrophy of the mucus-secreting cells.
|
Review Lung Histology
Slide No. 24 Lung
[DigitalScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
|
|
Gross Questions
Screen shot and annotate:
- hilum of the lung
- examples of airways and abnormal lung tissue (describe briefly the abnormal findings); and
- any near-normal or normal appearing lung tissue.
VM Image Questions
Annotate by screen shots:
- normal appearing lung tissue
- larger blood vessels and airways;
- examples of airway epithelium and airway smooth muscle; and
- examples of acute bronchiolitis and intraluminal necrotic and inflammatory debris.
539-1a. What is the differential diagnosis based on initial clinical presentation?
539-1b. What does the laboratory test suggest?
539-1c. What is the final diagnosis based on the history and gross and microscopic findings?
--ANSWER--
539-2. Which of the following genes is most frequently mutated in this disease?
- APC
- CFTR
- COL3A1
- FMR1
- LDLR
--ANSWER--
539-3. Which of the following best accounts for the pulmonary findings in this patient?
- Decreased chloride secretion in respiratory epithelium
- High-volume surface fluid layer coating respiratory mucosa cells
- Hyperplasia of bronchial smooth muscle
- Hypoplasia of bronchiolar cartilage
- Increased water and sodium secretion in respiratory epithelium
--ANSWER--
539-4. Which of the following is most commonly found in patients with this disease?
- Cherry red macula
- Hepatosplenomegaly and bone lesions
- Increased plasma LDL
- Light colored hair and skin
- Pseudomonas aeruginosa infection
--ANSWER--
CASE NUMBER 601 (virtual slide in part 2 below)
Clinical History: A 44-year-old man has developed increasing arthritis pain, swelling of the feet, and reduced exercise tolerance over the past 3 years. He has smoked 1 pack of cigarettes per day for 20 years. Physical exam reveals metallic gray pigmentation of the sun-exposed skin on his face and bilateral swelling of the first and second metacarpophalangeal joints. His liver percussed to a span of 13 cm (normal 10.5 cm).
Laboratory studies include serum glucose of 201 mg/dL, creatinine 1.1 mg/dL and elevated serum iron of 175 mg/dL (normal, 50-150 mg/dL).
601-1. Which additional lab tests would you order?
- Transferrin saturation
- Chest X-ray
- MRI of the foot
- Joint aspirate
- Glucose tolerance test
--ANSWER--
Clinical History (continued): Labs are drawn and values are as follows:
Test |
Value (ref. range in parentheses) |
Transferrin saturation |
88% (20-50%) |
Serum ferritin |
650 ng/mL (23-336 ng/mL) |
TIBC |
200 (250370 µg/dL) |
601-2. Which of the following best explains the elevated ferritin level?
- He has iron deficiency
- Excess ferritin comes from cigarette smoke
- This is a consequence of early diabetes
- There is an excess of iron in the body
- He is in renal failure
--ANSWER--
Clinical History (continued): A chest radiograph shows bilateral pleural effusions, pulmonary edema, and cardiomegaly. Abdominal CT confirms hepatomegaly. He undergoes a liver biopsy, and the microscopic appearance of a biopsy specimen stained with Prussian blue is shown.
slide (courtesy of UMich)
[DigitalScope]
Image Gallery:
Summary of Radiographic and Gross Findings
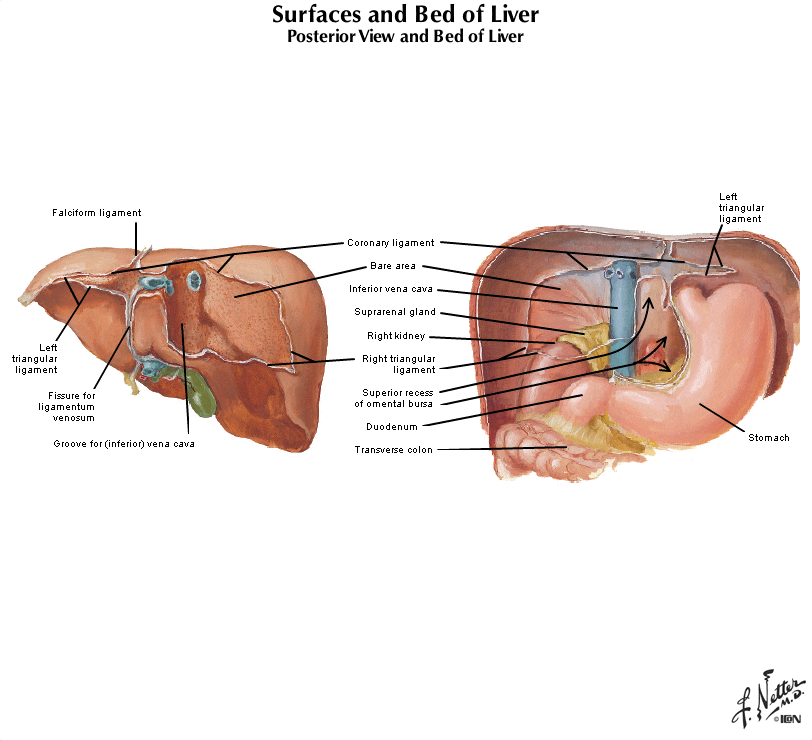
A chest radiograph shows bilateral pleural effusions, pulmonary edema, and cardiomegaly. On non-contrast CT, the liver is enlarged and shows diffusely increased density. The hepatic vasculature and biliary tree appear conspicuous due to their relative hypodensity. Gross specimens from the autopsy of a patient with the same disease show brown discoloration of the liver (top), pancreas (lower left), and a lymph node (lower right).
|
Summary of Microscopic Findings
The low power view shows liver cirrhosis with regenerative hepatic nodules surrounded by dense fibrosis. The hepatocytes show a faint brown discoloration on this low power view. Higher power magnification shows abundant granular brown pigment within hepatocytes and bile duct epithelium. Even higher power magnification shows hepatocytes with abundant dense brown granular pigment. The Prussian blue stain shows abundant intracellular iron.
|
Review Liver Histology
Slide No. 3 Liver
[WebScope]
The liver is the organ that metabolizes nutrients received from the digestive tract. These nutrients and processed by tissue hepatocytes which are large polygonal cells. The hepatocyes are separated by portal triads. The triads consist of an artery, a vein and a bile duct. The bile duct is lined by cuboidal epithelium. The artery has a muscular wall and a flat endothelial lining. The sinuses are well defined and contain a small amount of blood.
|
|
|
Radiology Questions
- Annotate the chest x ray highlighting the pleural effusion (s).
- After evaluating the transverse CT scan, label the liver, spleen, and one additional bonus landmark that helps you orient yourself to the image
Gross Questions
VM Image Questions
- Screen shot and annotate at low power a representative image that best describes the overall tissue injury/repair process present in the liver (hint: this is a general pattern of chronic injury);
- at high magnification find a cluster of hepatocytes and describe what you see; and
- identify the intracellular material that has accumulated in the hepatocyte. How does the Prussian blue stain help in our differential diagnosis?
601-2. Why is the ferritin level elevated?
- He has iron deficiency
- Excess ferritin comes from cigarette smoke
- This is a consequence of early diabetes
- There is an excess of iron in the body
- He is in renal failure
--ANSWER--
601-3a. What is the differential diagnosis based on the initial presentation (arthritis, foot swelling, etc)?
601-3b. Based on the physical exam?
601-3c. What do the laboratory tests reveal?
--ANSWER--
601-3d. What is the final diagnosis and why?
601-4. Which of the following genes is most likely mutated in this patient?
- ATP7B
- CFTR
- FMR1
- HFE
- NPC1
--ANSWER--
CASE NUMBER 503
(no virtual slide for this case)
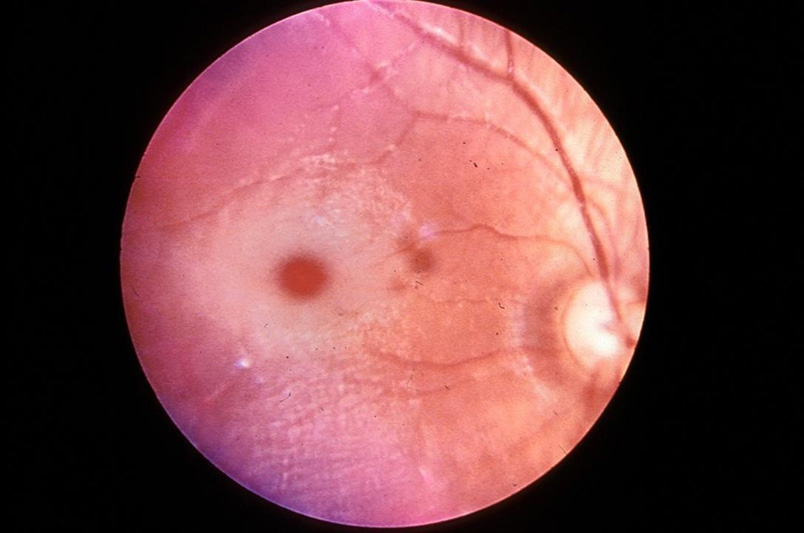
Clinical History: A mother brought her 3-month-old infant to the pediatrician because the child had been alternately crying inconsolably or lying down listlessly; vomiting for the last 3 days, and had a mild fever. Physical exam reveals cherry red maculas. CSF analysis shows elevated protein levels. Gene sequencing reveals a mutation in the alpha-subunit of hexosaminidase A.
Image Gallery:
Fundoscopy image questions:
- Screen shot and annotate the significant findings on the fundoscopy.
Electron microscopy image questions:
- Describe the findings on ultrastructural evaluation. What might be your differential diagnosis for the changes seen?
503-1. What might be your differential diagnosis for the changes seen?
--ANSWER--
503-2. This disease is classified as which of the following?
- Glycogenosis
- Mucolipidosis
- Mucopolysaccharidosis
- Sphingolipidosis
- Sulfatidosis
--ANSWER--
CASE NUMBER 7
(no virtual slide for this case)
Clinical History: A 48-year-old woman presents to the emergency department in labor. She has had no prenatal care. Delivery of the full-term infant is uncomplicated. An image of the neonate is provided.
Image Gallery:
Summary of Clinical Findings
The palpebral fissures slant upwards, the nasal bridge is flattened and the mouth is open with a protruding tongue.
|
7-1a. What is the differential diagnosis based on the clinical findings?
7-1b. Based on the cytogenetics?
--ANSWER--
Clinical History (continued): Cytogenetics is performed and shows that some of the patients cells have a normal karyotype(46,XX) and others are 47,XX, +21
7-2. Which of the following processes best accounts for this patients karyotype?
- Amplification
- Chromosomal deletion
- Lyonization
- Mosaicism
- Premutation
--ANSWER--
7-3. Which of the following is the most likely etiology of this finding (ie. answer to question 2)?
- Amplification of the short arm of chromosome 21
- Excess trinucleotide repeats
- Meiotic nondisjunction
- Mitotic nondisjunction
--ANSWER--
7-4. Which of the following is most strongly associated with risk of having a child with this disease?
- Advanced maternal age
- In utero alcohol exposure
- Insufficient folate
- Oligohydramnios
- Toxoplasma infection
--ANSWER--
7-5. For which of the following is this patient at greatest risk?
- Alzheimer disease
- Hyperlipidemia
- Hypocalcemia
- Infertility
- Retinoblastoma
--ANSWER--
GENETIC DISORDERS Review Items
Key Vocabulary Terms (click here to search any additional terms on Stedman's Online Medical Dictionary)
LEARNING OBJECTIVES
Goal 1: Genetic Mechanisms of Developmental and Functional Abnormalities
Apply knowledge of the genetic mechanisms of disease to discuss how changes in the genome can cause developmental and functional abnormalities at the cellular, tissue and organism levels.
- Objective 1: Types of Mutations
Describe different types of mutations that can occur in human disease, and discuss how each of these can produce abnormalities in DNA transcription, and/or alterations in the type or amount of protein produced.
- Objective 2: Inheritance Patterns
Compare and contrast, with examples, the inheritance patterns of different types of Mendelian disorders.
- Objective 3: Genetic Diseases of Enzyme Function
Provide examples of genetic diseases associated with abnormal enzyme function, as opposed to those that produce abnormal structural or other non-enzyme proteins.
- Objective 4: Chromosomal Abnormalities
Discuss mechanisms that result in developmental abnormalities involving abnormal chromosomal number and provide examples of diseases associated with trisomies or chromosomal deletions.
- Objective 5: Multifactorial Inheritance and Environmental Factors
Discuss, with examples, disorders associated with multifactorial inheritance and describe how environmental factors can interact with genetic factors to produce disease.
- Objective 6: Non-classical Inheritance
Describe the pathophysiologic mechanisms that result in disorders of a non- classic inheritance and give clinical examples of each.
|