Website Cases:
Additional case (NOT assigned):
CASE NUMBER 126
[DigitalScope]
Clinical History: A 50-year-old woman presented to her primary care physician with a 2-month history of increasing dyspnea and unexplained weight loss. She had no history of smoking. Chest X-ray revealed a 5 cm right upper lobe mass. While she was waiting in radiology for a staging CT, she suddenly collapsed. She could not be resuscitated. Gross and microscopic images from the autopsy are provided.
126-1. What is the differential diagnosis?
Image Gallery:
The lungs were remarkable for a 5 cm mass in the right upper lobe. The cut surfaces were friable and yellowish-gray. Regional lymph nodes were filled with similar necrotic tumor.
|
The tumor tissue consists of glandular structures with very large nuclei which are often arranged in several layers. The nuclear to cytoplasmic ratio is low. There are several mitoses and the stroma contains increased amounts of collagen. Well differentiated adenocarcinomas, with a glandular pattern like this one, are uncommon in the lung.
|
Review Lung Histology
Slide No. 24 Lung
[DigitalScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
|
|
Radiology image questions:
Take a screenshot of the chest X ray and annotate:
- the mass and the lateral borders of the heart.
On the axial chest CT, take a screenshot and annotate:
- the ascending and descending thoracic aorta,
- the carina and the mass.
Gross image questions:
- Take a screenshot and annotate the lesion.
- Describe the lesion (e.g., is it homogeneous or heterogeneous?)
- What does the gross suggest you will see on the histology?
VM image questions
Take a screenshot and identify:
- areas of normal lung and the pleural surface;
- at scanning magnification, highlight the abnormal/pathologic areas; and
- describe the lesion and some features which help you assess whether the lesion is benign, reactive or malignant.
126-2. Which of the following is most accurate regarding this diagnosis?
- It arises from neuroendocrine cells
- It is the most common pulmonary malignancy in non-smokers
- It is typically hilar
- Its incidence has decreased markedly in the last 20 years
- Mutations in ROS1 are common
126-3. Which of the following is most likely mutated in this patient?
- ALK1A
- BRAF
- EGFR
- HER2
- KRAS
126-4. Which of the following is most commonly associated with this malignancy?
- Cushing syndrome
- Hypercalcemia
- Migratory thrombophlebitis
- Myasthenic syndrome
- Polymyositis
CASE NUMBER 511 - slide courtesy of UMich
[DigitalScope]
Clinical History: A 67-year-old man presented to his primary care physician with a two-month history of fatigue and weight loss of ten pounds. Clinical history was relevant for a 60-pack-year smoking history and a 5-year history of hypertension and obstructive pulmonary disease. The patient died shortly after diagnosis. A section from the lung mass is provided.
511-1. What is the differential diagnosis?
Image Gallery:
The chest CT shows a large mass in the right lung and hilum. The second image is a CT of the abdomen that shows multiple lucent lesions in the liver and spleen, consistent with metastatic carcinoma.
|
The cytologic specimens show clusters of atypical cells with minimal cytoplasm. There is nuclear molding. The chromatin is mostly fine without a large nucleolus. The histologic section shows a portion of lung with a focus of bronchial cartilage and respiratory epithelium as well as minimal normal lung parenchyma. There is a mass lesion composed of an infiltrative population of small hyperchromatic cells with minimal cytoplasm. Mitotic figures are readily apparent. Higher magnification shows fine chromatin and nuclear molding. A lymph node with anthracotic pigment is present.
|
Review Lung Histology
Slide No. 24 Lung
[DigitalScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
|
|
Radiology questions:
In the chest CT, take a screenshot and annotate:
- the mass, ascending and descending thoracic aorta,
- main pulmonary artery and
- a pleural effusion.
In the abdominal CT, take a screenshot and annotate:
- lesions in the liver and spleen.
VM questions:
- Describe the architectural growth pattern of the mass seen at medium power.
- Using higher power, take a screenshot and annotate:
- areas of necrosis;
- a mitotic figure; and
- examples highlighting the morphologic characteristics of this tumor (describe these characteristics briefly).
511-2. Which of the following is most accurate regarding this disease?
- Biologic behavior is typically indolent
- Cells show a neuroendocrine phenotype
- Hypercalcemia is commonly diagnosed in these patients
- Incidence among non-smokers is rising
- Surgical resection is standard therapy
511-3. Which of the following is most commonly associated with this disease?
- Carcinoid syndrome
- Horner syndrome
- Hypoglycemia
- Nephrotic syndrome
- Syndrome of inappropriate antidiuretic hormone (SIADH) secretion
511-4. Which of the following has the strongest association with cigarette smoking?
- Adenocarcinoma
- Adenosquamous carcinoma
- Carcinoid tumor
- Pulmonary hamartoma
- Small cell carcinoma
CASE NUMBER 603
[DigitalScope]
Clinical History: A 62-year-old man has a 60-pack-year smoking history and a 10-year history of cough productive of copious mucopurulent sputum. Over the past 6 months, he has developed progressive dyspnea. Physical examination shows bilateral pedal edema and a soft but enlarged liver. A chest radiograph shows bilateral pleural effusions and a prominent heart border on the right side. Arterial blood gas determinations show:
- PO2 of 60 mm Hg
- PCO2 55 mm Hg
- pH 7.31
- HCO3- 28 mEq/L.
The patient is intubated and placed on a ventilator, and he requires increasing amounts of oxygen; however, despite supportive care, the patient expires. An autopsy is performed.
603-1. What is the differential diagnosis?
Image Gallery:
Gross examination of the airways demonstrates hyperemia with mucostasis. The long bronchus depicted in the first gross image is filled with tan, thick mucus. The second gross image demonstrates fibrosis of the bronchiolar wall.
|
The first microscopic image demonstrates goblet cell metaplasia with in the subepithelial seromucus glands in the airway wall. There is also an increase in the size/number of these glands. Patients with chronic bronchitis tend to have an elevated Reid index (Reid index - can be evaluated in airways with cartilage (bronchi) . RI = thickness of the mucus producing glands/the thickness of the bronchus from basal lamina to cartilage)
The second microscopic image depicts a bronchus with an elevated Reid Index. The third microscopic images shows ciliated pseudostratified respiratory epithelium with goblet cell metaplasia, and there is mild thickening of the basal lamina (basement membrane)
The third microscopic image depicts collections of smoker’s macrophages
|
Review Lung Histology
Slide No. 24 Lung
[DigitalScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
|
|
Gross image questions:
In the first gross image:
- identify and annotate the lung tissue and airway in the photo.
- Identify the abnormal material in the airway.
- What might your differential be based on what you see?
In the second image:
- highlight areas of emphysema and annotate one of the airways.
- What is significant about the gross appearance of the airway?
Microscopic image questions:
In an annotated screenshot of micro image 1, identify:
- the airway epithelium,
- submucosal glands,
- focus of inflammation.
What is the significant pathologic finding in micro image 2?
In micro images 3 and 4 identify:
- a goblet cell and
- "smokers'" type macrophages.
603-2. At autopsy, which of the following microscopic findings is most likely to be characteristic of his underlying pulmonary disease?
- Infiltrates of eosinophils
- Extensive interstitial fibrosis
- Granulomas in bronchovascular distribution
- Carcinoma filling lymphatic spaces
- Hypertrophy of bronchial submucosal glands
603-3. Which of the following is the most likely consequence of long-term disease?
- Atypical adenomatous hyperplasia
- Horner syndrome
- Pulmonary hypertension
- Sicca syndrome
- Small cell carcinoma
CASE NUMBER 452
[DigitalScope]
Clinical History: A 45-year-old man presented to his primary care physician with a 6-week history of non-productive cough. Over the last month or so, he had lost 15 pounds and occasionally experienced hemoptysis. He was originally from India, but moved to the United States nine years ago. Physical exam revealed harsh breath sounds with crackling rales over the right posterior lung base. A chest x-ray and CT were performed. Samples were taken for culture analysis; however, as he was leaving the doctor’s office, he experienced severe coughing with massive hemoptysis and died. Gross and microscopic images and laboratory findings are provided.
452-1. What is the differential diagnosis?
Image Gallery:
The lungs are heavy and have fibrous pleural adhesions. A large cavity containing caseous material is found in the apex of the right lung. The entire right upper lobe is affected. In the left upper lobe there is an area of consolidation, which exuded creamy, yellow-gray, caseous material from the cut surface. (Case image courtesy of A.Prof Frank Gaillard, Radiopaedia.org. From the case rID: 8633) |
This section shows many foci of caseous necrosis. At low power, you can see at least three of these foci with central necrosis. Scattered throughout are multinucleated giant cells. At higher power, you can see a marked proliferation of histiocytes around the caseous foci which contain neutrophils and necrotic debris.
|
Review Lung Histology
Slide No. 24 Lung
[DigitalScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
|
|
Radiology image questions:
In the chest CT, take a screenshot and annotate an area of consolidation.
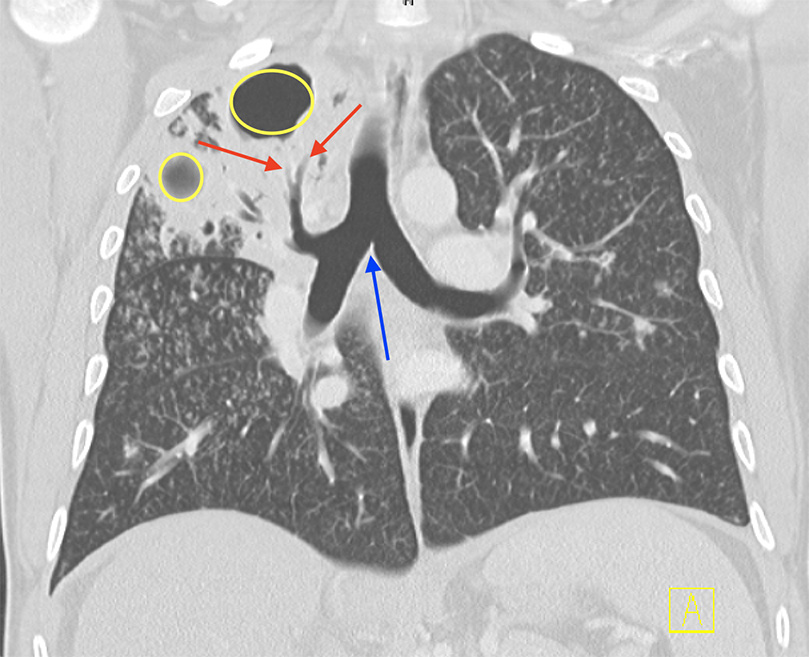
In the coronal CT:
- take a screenshot and annotate two cavitary lesions, an area of bronchiectasis and the carina.
- Does the background lung parenchyma look normal?
- If not, what do you see?
Gross image questions:
- Annotate in gross image areas of normal and abnormal lung.
- In the abnormal areas, describe the changes and provide a differential based on what you see.
VM image questions:
- Using a screenshot and annotation, identify and describe the pattern of inflammation.
452-2. Which of the following cells does Mycobacterium tuberculosis typically infect?
- B cells
- Cytotoxic T cells
- Macrophages
- Natural killer cells
- T helper cells
452-3. Immunity to M. tuberculosis is primarily mediated by which of the following?
- Plasma cells
- Natural killer cells
- TH1 cells
- TH2 cells
- TH17 cells
452-4. Which of the following is following is associated with primary tuberculosis infection?
- Asteroid bodies
- Cavitary lesions
- Ghon complex
- Hemoptysis
- Masson bodies
CASE NUMBER 127
[DigitalScope]
Clinical History:33-year-old woman presents to her primary care physician with a 2-year history of gradually worsening dry cough and dyspnea. She has never smoked and works in an office job. Over the last 6 months, she has noticed a low-grade fever and occasional night sweats. A chest X-ray and high resolution CT were performed. Laboratory testing is significant for elevated serum and urinary calcium. A PPD test is negative. A lung biopsy is performed.
Differential diagnosis questions:
127-1a. What is the differential diagnosis based on the clinical presentation?
127-1b. What is the differential diagnosis based on the radiologic and laboratory findings?
127-1c. What is the final diagnosis?
ANSWER
Image Gallery:
Plain radiograph: There is are profuse bilateral small pulmonary nodules, most numerous in the upper and middle lung zones in association with symmetrical bilateral hilar lymphadenopathy.
High resolution CT: There are diffuse bilateral multi-focal micronodules distributed along perilymphatic areas, subpleural regions, interlobular septa, and bronchovascular bundles. (Case images courtesy of Radiologykey.com). |
Abundant noncaseating granulomas are seen in the pulmonary interstitium (as opposed to involving air spaces), particularly around bronchioles and pulmonary venules (lymphatic distribution). Rare granulomas show necrosis. Although sarcoidosis is usually referred to as having non-necrotizing granulomas, there can be focal necrosis as there is in this case. However, the necrosis is noncaseating, which helps point us away from tuberculosis to sarcoidosis.
|
Review Lung Histology
Slide No. 24 Lung
[DigitalScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
|
|
Radiology image questions:
- Describe the chest X-ray and CT findings. Is the process diffuse or localized?
- How are the lesions distributed in the lung parenchyma?
VM image questions:
127-2.Which of the following would likely be seen in this patient’s pulmonary function tests?
- Decreased FVC, increased FEV1
- Decreased FVC, decreased FEV1
- Increased FVC, decreased FEV1
- Increased FVC, increased FEV1
ANSWER
127-3. Which of the following is thought to be central to the pathogenesis of this disease?
- B cells
- CD4+ T cells
- CD8+ T cells
- Eosinophils
- Neutrophils
ANSWER
127-4. Which of the following is a characteristic finding in patients with this disease?
- Erythematous nodules on the anterior legs
- Deposits of complement in pulmonary vessel walls
- Destruction of alveolar walls without fibrosis
- Plexiform vascular lesions
- Sheets of intra-alveolar macrophages with dusty-brown pigment
ANSWER
127-5. Which of the following is the proposed mechanism for elevated serum and urinary calcium?
- Antibodies cross-reacting with the parathyroid hormone receptor
- Bone destruction by intracortical granulomas
- Complement deposition in the parathyroid gland
- Parathyroid hormone-related peptide release by Th1 cells
- Vitamin D production by macrophages
ANSWER
LUNG PATHOLOGY Review Items
Key Vocabulary Terms (click here to search any additional terms on Stedman's Online Medical Dictionary)
RESPIRATORY SYSTEM LEARNING OBJECTIVES
Goal 1: Acute Respiratory Distress Syndrome
Apply knowledge of physiology, cellular biology, inflammation and histology to explain the clinical and pathophysiological consequences of acute lung injury.
Objective 1: Acute Respiratory Distress Syndrome
Describe the risk factors, etiology, clinical presentation, pathologic features and natural history of acute respiratory distress syndrome.
Goal 2: Obstructive Diseases of the Lung
Apply knowledge of the genetic and environmental factors leading to cell injury to explain the clinical and pathophysiological consequences that result in obstruction to airflow.
Objective 1: Emphysema
Describe the role of smoking in emphysema; name the four (4) different types of emphysema, which is most common, and which lobes are most involved in centrilobular emphysema.
Objective 2: Bronchiectasis
Explain the gross morphologic changes associated with bronchiectasis and name diseases that may lead to bronchiectasis.
Objective 3: Chronic Bronchitis
Describe the predisposing factors, etiology, clinical presentation, pathologic findings and disease course of chronic bronchitis.
Objective 4: Asthma
Compare and contrast the different types of asthma in terms of risk factors, etiology, clinical presentation, pathologic findings and disease course.
Goal 3: Restrictive Diseases of the Lung
Apply knowledge of the genetic and environmental factors leading to cell injury to explain the clinical and pathophysiological consequences that result in restriction to airflow.
Objective 1: Fibrosing Diseases and Pneumoconiosis
Compare and contrast the clinicopathologic features of the fibrosing diseases of lung.
Objective 2: Pneumoconiosis
Compare and contrast the clinicopathologic features of the different types of pneumoconioses.
Objective 3: Granulomatous Diseases
Compare and contrast the granulomatous diseases of the lung in terms of epidemiology, clinical presentation, pathologic findings, systemic effects and natural history.
Goal 4: Vascular Diseases of the Lung
Apply knowledge of the structure and function of blood vessels to explain the pathogenesis, clinical manifestations, and pathologic findings in pulmonary embolism, pulmonary hypertension, and diffuse pulmonary hemorrhage syndromes.
Objective 1: Clinical Features of Pulmonary Embolism
Compare and contrast the clinical manifestations, radiographic and pathologic findings, and potential consequences of pulmonary embolism in terms of single versus multiple and small versus large emboli.
Objective 2: Conditions Predisposing to Pulmonary Embolism
List the factors, including underlying conditions, which can impact the incidence and clinical significance of pulmonary embolism.
Objective 3: Pulmonary Hypertension
List the structural cardiopulmonary conditions that are frequently associated with pulmonary hypertension.
Objective 4: Conditions Contributing to Pulmonary Hypertension
Explain how each of the following cardiopulmonary conditions contributes to pulmonary hypertension: increased pulmonary blood flow or pressure, increased pulmonary vascular resistance, or left heart resistance to blood flow.
Objective 5: Goodpasture Syndrome and Granulomatosis with Polyangiitis (Wegener Granulomatosis)
Compare and contrast the clinical manifestations, pathogenesis, and pathologic findings in Goodpasture syndrome and granulomatosis with polyangiitis (Wegener granulomatosis).
Goal 6: Pulmonary Infection
Apply knowledge of the local pulmonary defense mechanisms and systemic host resistance to infection to discuss pathogenesis, classification, clinical manifestations, and pathologic findings in lower respiratory tract infections in immunocompetent and immunocompromised hosts.
Objective 1: Classification of Pneumonia by Agent
Describe the classification of pneumonias by clinical setting and name the common etiologic agents for each category.
Objective 2: Clinical Features of Pneumonia
Compare and contrast the clinical presentation and manifestations, gross and microscopic pathology, prognosis, and potential complications for each category of pneumonias.
Objective 3: Categorization of Pneumonia
Define bronchopneumonia, lobar pneumonia, and atypical pneumonia/interstitial pneumonitis and compare and contrast the common etiologic agents and gross microscopic findings for each.
Objective 4: Tuberculosis
Compare and contrast the clinical presentation, and gross and microscopic findings in primary, secondary/reactivation, and miliary tuberculosis.
Objective 5: Aspiration Pneumonia
Name risk factors for aspiration pneumonia and describe the pathology, prognosis, and potential complications.
Objective 6: Lung Abscess
Define lung abscess in terms of pathogenesis, typical microorganisms, clinical presentation and course, and pathologic findings.
Objective 7: Fungal Pneumonia
Compare and contrast the causative agents, geographic locations, clinical presentation, and pathologic findings in chronic pneumonia caused by fungal organisms
Objective 9: Features of Pulmonary Infections in the Immune-compromised and Immunocompetent
Discuss the differences in clinical presentation and etiologic agents of pneumonia in immunocompetent versus immunocompromised hosts.
Goal 7: Lung Neoplasia
Apply knowledge of the molecular basis of neoplasia to describe clinical presentation, biologic behavior, morphologic appearance, classification, diagnosis, prognosis and targeted therapy of lung neoplasms.
Objective 1: Lung Neoplasms
Describe the common locations and clinical presentation for the different types of lung cancer.
Objective 2: Morphologic Features of Lung Neoplasms
Identify key gross and histopathologic features that help differentiate between small cell, adenocarcinoma, and squamous cell carcinoma.
Objective 3: Metastatic Carcinoma to the Lung
Describe features that favor the diagnosis of metastatic carcinoma over a primary lung tumor.
Objective 4: Genetics of Lung Cancer
Describe the contribution of specific genetic mutations that contribute to particular lung cancers and explain how these mutations affect therapeutic decisions.
Objective 5: Environmental Factors Predisposing to Lung Cancer
Explain the environmental factors that predispose to the development of lung cancer and illustrate how these factors interact with genetic factors in the development of cancer.
|